| Issue |
SICOT-J
Volume 12, 2026
|
|
|---|---|---|
| Article Number | 15 | |
| Number of page(s) | 9 | |
| Section | Hip | |
| DOI | https://doi.org/10.1051/sicotj/2025065 | |
| Published online | 15 April 2026 | |
Original Article
Long versus short cephalomedullary femoral nail for treatment of unstable intertrochanteric fractures: A single-blinded randomized controlled study
Orthopaedic Surgery Department, Faculty of Medicine, Ain Shams University, 38 Abbassia, 11591 Cairo, Egypt
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
22
August
2025
Accepted:
8
December
2025
Abstract
Background: ITF are extracapsular proximal femoral fractures that occur in both younger and older populations, with a higher prevalence among females. They account for most hip fractures, reaching 44.1%. The Elderly are at risk with an increased first-year mortality risk reaching up to 30%. This research aimed to compare the functional outcomes, effectiveness, and safety profile of long as opposed to short cephalomedullary nails (CMNs) in the management of unstable ITF in elderly individuals aged >60 years. Methods: This single-blinded randomized controlled research was carried out on 30 participants aged >60 years old, both sexes, with unstable ITF. Participants were categorized into two groups (GPs): GP A: had a long cephalomedullary nail (LCMN), and GP B: had short cephalomedullary nail. Results: Mean hospital stay length, period of surgery, operative blood loss, and the incidence of transfusion requirements were higher in GP A, yet no significant difference was observed. Functional outcomes, union and complication rates were comparable between the two GPs. Conclusions: Irrespective of the length, CMNs are suitable for the treatment of unstable ITF, aiming to achieve early mobility and satisfactory functional outcome. Further large-sampled RCTs need to be conducted comparing both GPs based on more recent CT-based classification systems with osteoporosis considered.
Key words: Intertrochanteric fractures / Cephalomedullary femoral nails / AO/OTA classification / Harris hip score
© The Authors, published by EDP Sciences, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Intertrochanteric femoral fractures (ITF) represent extra-capsular fractures extending between the greater (GT) and lesser trochanters (LT) [1]. Due to its trabecular nature, the elderly are subjected to osteoporotic fractures with an increased first-year mortality risk reaching up to 30% compared to femoral neck fractures [2].
ITF accounts for most hip fractures, reaching up to 44.1% [3]. They are treated with internal fixation, whether by dynamic hip screws (DHS) or cephalomedullary nails (CMN), with the latter being the most frequently used, for both stable and unstable fractures [4].
ITFs are classified according to their stability into stable and unstable. Stability is assessed by an intact calcar femoral, decreased lateral wall thickness below 20.5 mm, subtrochanteric extension, and the reverse oblique subtype [5, 6].
CMN are classified into long and short, with a length of 250 mm as a cut-off, and short nails not crossing the femoral isthmus [7]. Across the literature, LCMN and SCMN were comparable biomechanically, with LCMN having the theoretical advantage of increased stability in ITF with subtrochanteric extension and a lower incidence of periprosthetic diaphyseal fractures. However, nail-femur curvature radius mismatch might lead to anterior cortex perforation, which could be avoided by proper nail size and posterior entry point [8].
The dimensions of the LT may also influence the choice of CMN, as fracture fragments located inferior to the base of the LT by 40 mm may render the SCMN to fail with subsequent distal cortical plastic deformation [9]. In contrast, SCMN had shorter surgical duration, minimized blood loss, decreased transfusion requirements, and decreased costs [10].
This study aimed to compare the operative time, functional outcome, efficacy, and safety profile of LCMN and SCMN in treating unstable ITF fractures in patients over 60 years old.
Materials and methods
This single-blinded randomized research was carried out on 30 participants aged >60 years old, both sexes, with unstable ITF. The investigation was executed from December 2023 to December 2024, after approval from the Ethical Committee of Ain Shams University Hospitals, Cairo, Egypt (FMASU MS 699/2023). Retrospectively registered in PACTR (PACTR202506720274898) due to logistical causes. All participants provided written informed consent before enrolment.
Exclusion criteria were patients with stable intertrochanteric fractures, unstable intertrochanteric fractures with subtrochanteric extension, associated hip pathology, bedridden or immobile patients, pathological fractures secondary to malignant disease, previous ipsilateral hip surgeries, and extreme anteroposterior (AP) femoral bowing or deformity.
Randomization and blindness
Patients were randomized through a computer-generated random number table to assign participants with ITF into two groups: GP A Underwent treatment involving an LCMN, whereas those in GP B received a SCMN.
A thorough clinical evaluation and appropriate radiological investigations [X-rays and computed tomography (CT)] were performed for all participants.
Preoperative evaluation: modified Harris hip score (MHHS) was applied to estimate the baseline functional status and multiplied by 1.1 to calculate the pre-injury HHS [11].The Barthel index (BI), an indicator for the activity of daily living, was used to assess the independence of the patients before the fracture.
Surgical technique
Patients underwent spinal anesthesia and were positioned laterally with the affected limb on top. A trial of reduction was done to correct the anatomical alignment, angulation, and version of the proximal femur using fluoroscopy (Figure 1A). The whole affected lower limb was then sterilized with povidone iodine and draped from the iliac crest down toward the foot. Intravenous antibiotic; Cefazolin® is given 30 min before incision time in weight-adjusted dosing. The main surgeon stands facing the posterior aspect of the thigh with the assistant standing on the opposite side (Figure 1B). The GT is palpated (Figure 1C), and then a 5 cm incision proximal to the tip of the GT is made with a slight posterior inclination. Fractures were either closed or openly reduced. Reduction was aided by the use of bone hooks, pointed clamps, hohmans, and manual manipulation (Figure 1D).
 |
Figure 1 Surgical technique. |
After fracture reduction, an entry point is purchased using a cannulated awl just medial to the GT tip per company instructions (Figure 1E). Serial Reaming was done till reaching a suitable canal diameter, followed by nail placement, whether by LCMN or SCMN. GT fractures were addressed by either a cortical 6.5 mm screw or direct repair with ethibond® size 2 sutures. All nails were provided by ORTHOMED ® Company with SCMN length ranging from 180 to 240 mm and LCMN length ranging from 340 to 420 mm. Regarding the width, all nails, whether SCMN or LCMN, ranged in width from 10 mm to 13 mm according to the reamed canal diameter. All lag screws inserted were 10.5 mm in diameter and ranged from 90 to 115 mm in length. In 22 out of 30 cases, anti-rotation screws were utilized with a diameter of 6.5 mm and a length ranging from 80 to 105 mm. The remaining eight cases used endcaps instead of an anti-rotation screw. 4.8 mm Distal locking screws locked the nail distally.
Drains were utilized according to the amount of blood oozing. Total operative time was measured from the incision time to the start of skin closure. Blood loss was measured from suction devices, collected blood, and soaked dressings.
Postoperative management: prophylactic novel anticoagulants were offered to Guard against deep vein thrombosis. Intravenous Antibiotics were continued 48 h post-procedure to guard against infection, and appropriate analgesia was provided for all patients. Partial weight bearing was individualized based on patient factors, surgeon judgment, fracture pattern, and fixation quality. patients were discharged on oral Antibiotics after a Satisfactory wound status.
X-rays were done postoperatively with follow-up imaging at 3 weeks, 3 months, and 6 months intervals, monitoring for signs of union; assessed by callus formation and fracture line disappearance in 3 out of 4 cortices in AP and lateral views, and signs of complications. Functional outcomes were calculated using HHS and BI at 3 weeks, 3 months and 6 months.
The HHS is used to quantify functional outcome, with higher scores reflecting better clinical results. Scores were recorded and calculated during follow-up visits. The maximum attainable score is 100, and outcomes are interpreted as follows: scores <70 were considered indicative of a poor outcome; scores 70–80 were classified as fair, 80–90 as good, and 90–100 as excellent.
Outcome evaluation
Intraoperative variables, which compare operative duration, intraoperative blood loss, blood transfusion rate, and technical calculations including tip apex distance (TAD), nail length and width, reduction type, and the use of antirotation or endcap. Post-operative outcome, which includes duration of inpatient hospitalization and radiographic union, functional outcomes (HHS and BI) and complications covering radiographic parameters (non-union, implant failure, periprosthetic fracture, varus collapse, heterotopic ossification) and clinical outcomes (time to weight bearing, fracture related infection (FRI), hip pain, mortality), used to compare safety and efficacy between GPs.”
Statistical analysis
It was performed using SPSS version 26 (IBM Corp., Chicago, IL, USA). Quantitative variables were shown as mean ± standard deviation (SD), and the relation between GPs was assessed using the unpaired Student’s t-test. Categorical variables were shown as frequencies and percentages, and interpreted using the Chi-square test or Fisher’s exact test. A p-value of <0.05 was considered statistically significant.
Results
In this research, 40 participants were initially screened for inclusion criteria. Of these, 8 participants failed to fulfill the inclusion criteria, and 2 opted not to participate. A total of 30 remaining participants were randomly distributed across two equal GPs, with 15 participants in each GP. All participants ended follow-up and were incorporated into the final statistical analysis Figure 2.
 |
Figure 2 CONSORT flowchart of the enrolled patients. |
There was no statistically notable variation between the two GPs in terms of demographic characteristics and medical history. Regarding fracture patterns, the simpler fracture type (AO/OTA 31-A2) was the most prevalent in both GPs, with an incidence of 53.3% in GP A and 80% in GP B Table 1.
Comparison between two GPs regarding demographic data, medical history, and fracture assessment.
The majority of the patients in the long group reported a fair HHS score at 3 months compared to 5 patients in the short group. Regarding the BI score, an average of at least 15 more points was recorded more than the 3 weeks observed values. Eight patients (57.1%) in group A and seven patients (50%) in group B had good to excellent HHS scores at the time of the last follow-up, with an average of 76.86 ± 10.77 and 80.08 ± 11.21, respectively. Both groups had an average BI of at least 85 points Table 2.
Comparison between two GPs regarding operative data and at 3 weeks, 3, and 6 months follow-up.
Complications
During the 6-month follow-up period, 1 case died in each group within the first 35 days during their hospital stay due to poor general condition. From the LCMN, 1 patient was diagnosed with FRI within the first 3 weeks, which was managed by DIAR (debridement, irrigation, and implant retention) and later by antibiotic suppression till signs of union were observed at 3 months. In Group A, 2 patients complained of hip pain and had radiological signs of HO compared to 1 patient in the short group. They were prescribed (NSAIDS) indomethacin for 1 month and reported pain improvement Figure 3.
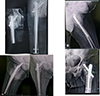 |
Figure 3 Heterotrophic ossification. |
Among the short GP, a patient presented with implant failure at a 2-month interval with avascular necrosis of the femoral head. There was significant varus collapse (>5°) with a z effect. Patient underwent implant removal and arthroplasty Figure 4.
 |
Figure 4 (A) (AO 31–A2.3) fracture pattern, (B) AP and lateral views 2 m later post-surgery showing AVN and varus collapse, and (C) CT 3D showing z effect. |
Two more patients in the short GP had varus collapse with the screw back out. One of which had additional screw breakage; both underwent implant removal.Only one patient in the long GP presented with varus collapse and screw cut-out Figure 5.
 |
Figure 5 Long CMN varus collapse and screw back out. |
Despite a higher complication rate with short CMN, no significant difference was found between groups Table 3.
Comparison between two GPs regarding the rate of complications.
Discussion
ITF are extracapsular fractures located in the proximal femur extending between the GT and LT [1].The most frequent mechanism of trauma was a trivial fall (80%), coinciding with the results produced by a similar RCT by Rahman et al. [12]. This was pointed out by the fact that 24 patients (80%) in this study had at least one co-morbidity, with 10 patients from both GPs being polymorbid, contributing to the fall and subsequent fracture.
As the most recent 2018 revision (AO/OTA) fracture and dislocation classification compendium reviewed, unstable ITF includes 31-A2.2, 31-A2.3, 31-A3.1, 31-A3.2, and 31-A3.3. The previous AO 31-A2.1 classification is left blank in the current classification and is no longer considered a valid secondary classification criterion due to the questionable contribution of LT to the stability [13]. That being said, Gotfried et al. [14] and Pradeep et al. [15] highlighted the relevance of the lateral wall integrity regarding the implant choice and therapeutic outcome. After traction x-rays, the majority of patients were presented with the simpler pattern AO 31-A2, and classified by Evans into type 1 fractures (with subtypes GP 3 and 4).
The total duration of hospital stay was comparable in both GPs. Nevertheless, the mean average time of operation was higher in the long CMN GP, possibly due to the nature of the procedure, where serial whole-length medullary reaming is required and the trials needed to place the distal screws ideally into their nail holes using the perfect circle technique or aiming jig with image fluoroscopy assistance. On the contrary, SCMN had a lower mean operative time as only partial medullary reaming is needed, and an aiming device is available for distal locking. Despite those mean differences, no significant differences were found between the two GPs compared to Boone et al. [16] where their results established a significant difference between the two GPs.
The mean estimated blood loss (236.67 mL) and transfusion necessity were higher in the long CMN GP, possibly due to the higher mean operative surgical time and the need for open reduction in those patients, as nearly half of the patients (7) had the more complex AO-31-A3 fracture subtype.
About two-thirds of the patients in both GPs were able to bear partial weight within 1 month, with an earlier proportion of mobile patients in the long GP with a ratio (1.4:1) within 2 weeks. At the final follow-up period, all patients achieved union apart from one patient in the short GP, who presented with implant failure, AVN and need for revision surgery. More than or equal to 50% of GPs achieved a good to excellent HHS score and above 80 Barthel scores. No marked difference was found between both GPs in terms of the functional outcome, concluding that both implants are valid options for unstable intertrochanteric fractures. Similar conclusions were reached by Ocku et al. [17].
No periprosthetic fractures were documented in our research, probably due to the time-dependent nature of this complication since the index procedure and all nails were locked distally, which may offer a protective advantage against refractures as portrayed by the retrospective study of Lindvall et al. [18] study.
The overall complication rate between both GPs was insignificant.
The limitations of the research include a relatively restricted sample population with a limited follow-up period, which may affect the validity and longitudinal relevance of the findings. Since it’s a surgical procedure, double blinding was not possible as the surgeon was exposed to the nail dimensions. The study was retrospectively registered in PACTR.
Irrespective of the length, CMN are suitable tools for the treatment of unstable ITF to achieve early pain-free mobility and functional outcome analogous to that of the pre-injury level. Despite higher mean values of total hospital stay, period of surgery, intraoperative blood loss, and blood transfusion in the LCMN, results were comparable regarding union, complication rates, and functional outcomes with no significant differences between the two groups. It’s advised to treat ITF on a case-by-case basis due to the heterogeneity of fracture patterns. It’s crucial to weigh the choice of implant; with a tendency to use SCMN in the elderly with a feeble nature to cut off operative time and blood loss relative to LCMN, which spans the femur, adding a biomechanical advantage in osteoporotic bones. We recommend larger randomized trials comparing short and long CMN, using modern fracture classifications (Kalia and Singh CT) and incorporating the Singh index to guide nail selection [19].
Funding
This research did not receive any specific funding.
Conflicts of interest
The authors declare they have no relevant financial or non-financial interests to report.
Data availability statement
Data are available from the corresponding author upon request.
Author contribution statement
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by A. A. A., H. A. and A. S. K. The first draft of the manuscript was written by A. A. A., and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Ethics approval
Ethical approval from the Ethical Committee, Ain Shams University Hospitals, Cairo, Egypt (Approval code: FMASU MS 699/2023).
Informed consent
An informed written consent was obtained.
References
- Noda M, Takahara S, Nishida R, et al. (2023) A demographic survey of pertrochanteric fractures based on the revised arbeitsgemeinschaft für osteosynthesefragen/orthopedic trauma association (AO/OTA) classification using 3D CT scan images. Cureus 15, 335–372. [Google Scholar]
- Ahn J, Bernstein J (2010) Fractures in brief: intertrochanteric hip fractures. Clin Orthop Relat Res 468, 1450–1452. [Google Scholar]
- Kim J-W, Kim D-H, Jang E-C, Lee Y-K, Koo K-H, Ha Y-C (2019) Mortality and its risk factors in nonagenarians after hip fractures. J Orthop Sci 24, 850–854. [Google Scholar]
- Zeelenberg ML, Plaisier AC, Nugteren LH, et al. (2024) Extramedullary versus intramedullary fixation of unstable trochanteric femoral fractures (AO type 31–A2): a systematic review and meta-analysis. Arch Orthop Trauma Surg 144, 1189–1209. [Google Scholar]
- Palm H, Jacobsen S, Sonne-Holm S, Gebuhr P (2007) Integrity of the lateral femoral wall in intertrochanteric hip fractures: an important predictor of a reoperation. J Bone Joint Surg Am 89, 470–475. [Google Scholar]
- Hsu C, Shih C, Wang C, Huang K (2013) Lateral femoral wall thickness: A reliable predictor of post-operative lateral wall fracture in intertrochanteric fractures. Bone Joint J 95, 1134–1138. [Google Scholar]
- Raval P, Ramasamy A, Raza H, Khan K, Awan N (2016) Comparison of short vs long anti-rotation in treating trochanteric fractures. Malays Orthop J 10, 22–28. [Google Scholar]
- Ostrum RF, Levy MS (2005) Penetration of the distal femoral anterior cortex during intramedullary nailing for subtrochanteric fractures: a report of three cases. J Orthop Trauma 19(9), 656–660. [Google Scholar]
- Lee WC, Chou SM, Tan CW, Chng LS, Yam GJM, Chua THI (2021) Intertrochanteric fracture with distal extension: When is the short proximal femoral nail antirotation too short? Injury 52, 926–932. [Google Scholar]
- Parola R, Maseda M, Herbosa CG, Konda SR, Ganta A, Egol KA (2022) Quality differences in multifragmentary pertrochanteric fractures [OTA 31A2.2 and 31A2.3] treated with short and long cephalomedullary nails. Injury 53, 2600–2604. [Google Scholar]
- Kumar P, Sen R, Aggarwal S, Agarwal S, Rajnish RK (2019) Reliability of modified Harris hip score as a tool for outcome evaluation of total hip replacements in Indian population. J Clin Orthop Trauma 10, 128–130. [Google Scholar]
- Rahman MAK, Siddiqui YS, Julfiqar M, Khan AQ, Sabir AB, Abbas M (2023) Short versus long proximal femoral nail in the management of intertrochanteric fractures – a comparative study. Int J Burns Trauma 13, 99–109. [Google Scholar]
- Song H, Hu SJ, Du SC, Xiong WF, Chang SM (2021) Sub-classification of AO/OTA-2018 pertrochanteric fractures is associated with clinical outcomes after fixation of intramedullary nails. Geriatr Orthop Surg Rehabil 12, 215–240. [Google Scholar]
- Gotfried Y (2004) The lateral trochanteric wall: a key element in the reconstruction of unstable pertrochanteric hip fractures. Clin Orthop Relat Res 90, 82–86. [Google Scholar]
- Pradeep AR, KiranKumar A, Dheenadhayalan J, Rajasekaran S (2018) Intraoperative lateral wall fractures during dynamic hip screw fixation for intertrochanteric fractures-Incidence, causative factors and clinical outcome. Injury 49, 334–338. [Google Scholar]
- Boone C, Carlberg KN, Koueiter DM, et al. (2014) Short versus long intramedullary nails for treatment of intertrochanteric femur fractures (OTA 31–A1 and A2). J Orthop Trauma 28, 96–100. [Google Scholar]
- Okcu G, Ozkayin N, Okta C, Topcu I, Aktuglu K (2013) Which implant is better for treating reverse obliquity fractures of the proximal femur: a standard or long nail? Clin Orthop Relat Res 471, 2768–2775. [CrossRef] [PubMed] [Google Scholar]
- Lindvall E, Ghaffar S, Martirosian A, Husak L (2016) Short versus long intramedullary nails in the treatment of pertrochanteric hip fractures: Incidence of ipsilateral fractures and costs associated with each implant. J Orthop Trauma 30, 119–124. [Google Scholar]
- Kalia RB, Arora SS, Sarkar B, Paul S, Singh S (2022) A comprehensive 3D CT based classification of intertrochanteric fracture. J Clin Orthop Trauma 30, 101–912. [Google Scholar]
Cite this article as: AbouelEla AA, Abdel-Azim H & Kotb AS (2026) Long versus short cephalomedullary femoral nail for treatment of unstable intertrochanteric fractures: A single-blinded randomized controlled study. SICOT-J 12, 15. https://doi.org/10.1051/sicotj/2025065.
All Tables
Comparison between two GPs regarding demographic data, medical history, and fracture assessment.
Comparison between two GPs regarding operative data and at 3 weeks, 3, and 6 months follow-up.
All Figures
|
Figure 1 Surgical technique. |
| In the text | |
|
Figure 2 CONSORT flowchart of the enrolled patients. |
| In the text | |
|
Figure 3 Heterotrophic ossification. |
| In the text | |
|
Figure 4 (A) (AO 31–A2.3) fracture pattern, (B) AP and lateral views 2 m later post-surgery showing AVN and varus collapse, and (C) CT 3D showing z effect. |
| In the text | |
|
Figure 5 Long CMN varus collapse and screw back out. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.