| Issue |
SICOT-J
Volume 12, 2026
|
|
|---|---|---|
| Article Number | 33 | |
| Number of page(s) | 14 | |
| Section | Lower Limb | |
| DOI | https://doi.org/10.1051/sicotj/2026030 | |
| Published online | 26 May 2026 | |
Review Article
Comparing outcomes for retrograde intramedullary nailing vs. antegrade intramedullary nailing for Femoral fractures – a systematic review and meta-analysis
1
East and North Hertfordshire NHS Trust, Stevenage, UK
2
Gradscape, London, UK
3
Medical University Plovdiv, Bulgaria
4
Northern Care Alliance NHS Foundation Trust, UK
5
Tamesdie and Glossop Integrated Care NHS Foundation Trust, UK
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
5
January
2026
Accepted:
3
April
2026
Abstract
Background: Distal femur fractures represent a small but clinically significant proportion of femoral injuries and are associated with high rates of complications, including non-union and revision surgery. Intramedullary nailing is a commonly employed fixation strategy, with both antegrade and retrograde approaches widely used in current practice. However, controversy persists regarding the optimal nail entry technique, particularly with respect to fracture healing, revision rates, and complications. This systematic review and meta-analysis aimed to compare clinical and radiological outcomes of antegrade versus retrograde intramedullary nailing for femoral shaft and distal femur fractures. Methods: This review was conducted in accordance with PRISMA guidelines and registered with PROSPERO (CRD420251274011). MEDLINE, EMBASE, and Cochrane databases were systematically searched for comparative studies evaluating antegrade and retrograde intramedullary nailing. Retrospective and prospective human studies reporting outcomes of union, revision, refracture, malunion, delayed union, operative time, and complications were included. Data extraction and quality assessment were independently performed, with risk of bias evaluated using the ROBINS-I tool. Meta-analysis was conducted using odds ratios (ORs) and weighted mean differences with 95% confidence intervals. Results: Five studies encompassing 1,479 patients were included, of whom 894 underwent antegrade nailing, and 585 underwent retrograde nailing. Antegrade nailing demonstrated a significantly lower rate of refracture following primary fixation compared with retrograde nailing (OR 31.41; 95% CI 4.45–221.80; p < 0.001). Revision rates were also significantly lower in the antegrade group (OR 1.76; 95% CI 1.21–2.58; p = 0.003). Retrograde nailing showed a higher overall union rate, although this did not reach statistical significance (p = 0.10). Rates of malunion, delayed union, non-union, operative time, and overall complications were comparable between groups, with moderate to substantial heterogeneity observed for several outcomes. Conclusion: Both antegrade and retrograde intramedullary nailing provide effective fixation for femoral shaft and distal femur fractures. Antegrade nailing is associated with significantly lower rates of refracture and revision, while retrograde nailing demonstrates comparable union outcomes. These findings suggest that antegrade nailing may offer advantages in selected patient populations, particularly elderly individuals, although the surgical approach should ultimately be guided by fracture pattern, patient factors, and surgeon expertise.
Key words: Antegrade approach / Retrograde approach / Femoral fracture
© The Authors, published by EDP Sciences, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Distal femur fractures account for 0.4% of all fractures and 3–6% of femur fractures [1]. Its age distribution is bimodal, with young people (20–30 years old with high energy injuries such as road traffic accidents) and elderly women (approximately 70 years old, with low energy injuries such as falls from standing height) being the most common [2, 3]. The goals of surgical fixation for these fractures are relative stability for diaphyseal fractures to initiate early mobilization, anatomical articular reduction, and blood supply preservation [4]. The non-union rate is quoted as high as 18–20% [5].
Compared to an eccentrically positioned plate and screws construct, intramedullary nails are load-sharing devices that stay close to the femoral axis and have better stress distribution. Nailing also requires a shorter operating time, less perioperative blood loss, and early patient mobilization [6].
One proven treatment for these fractures is retrograde nailing [7]. Prior research on the results of patients treated with retrograde nailing frequently included both young individuals with high-energy fractures and older patients with osteoporotic fractures [8, 9]. Retrograde intramedullary nailing was first used by Green in 1988 to treat distal femur fractures [10]. Its benefits include indirect reduction and internal fixation, which prevent excessive soft tissue dissection, periosteal blood supply interruption, and provide high union rates [11, 12].
Antegrade intramedullary nailing of the femur is an effective treatment for diaphyseal fractures [13]. The antegrade approach to femoral nailing is the favored way of fixation for the majority of surgeons due to its relative simplicity of patient posture (supine position with or without ipsilateral traction) and obvious surgical starting locations (piriformis fossa or greater trochanter, depending on nail design) [14].
A key consideration in antegrade intramedullary nailing is protection of the femoral neck, particularly in older osteoporotic patients, in whom reduced bone mineral density increases the risk of iatrogenic femoral neck fracture during entry point creation, reaming, or nail insertion. Malposition of the entry point, excessive insertion force, and implant–canal mismatch may increase stress within the proximal femur, predisposing to fracture. Given the substantial biomechanical forces transmitted through the femoral neck, meticulous surgical technique, appropriate implant selection, and careful intraoperative imaging are essential to minimize this risk [5].
The two methods for treating distal femur fractures – antegrade and retrograde intramedullary nailing – are compared and contrasted in this systematic study.
Search strategy and study design
A study protocol was developed and agreed upon by all authors prior to commencement. The review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [15]. A comprehensive electronic search was performed across MEDLINE (via PubMed), EMBASE, and the Cochrane Library, including the Cochrane Central Register of Controlled Trials.
Search terms were constructed using combinations of keywords and Medical Subject Headings (MeSH), including: (“femoral shaft fracture” OR “distal femur fracture”) AND (“antegrade intramedullary nailing” OR “retrograde intramedullary nailing”) AND (“union” OR “non-union” OR “revision” OR “malunion” OR “post-operative fracture”). Reference lists of included studies were manually screened to identify additional relevant articles.
Eligibility criteria
Studies were eligible for inclusion if they directly compared antegrade and retrograde intramedullary nailing for femoral shaft or distal femur fractures and reported at least one predefined clinical or radiological outcome. Both retrospective and prospective studies involving human participants were included. Exclusion criteria comprised biomechanical or cadaveric studies, case reports, narrative reviews, editorials, non-English publications, and studies lacking full-text availability.
Primary outcomes were fracture union, revision surgery, and refracture following index fixation. Secondary outcomes included operative time, mobility-related outcomes, and overall complication rates. The review was prospectively registered with PROSPERO (CRD420251274011).
Data extraction and quality assessment
Data extraction was independently undertaken by four reviewers (M.I.K., A.S., T.M., and N.S.) using a standardized extraction form. Extracted data were cross-checked by senior authors (K.R., K.A., and P.M.) to ensure accuracy. Information collected included study characteristics, patient demographics, fracture type, surgical technique, follow-up duration, and reported outcomes.
Risk of bias was assessed independently by two reviewers (K.R. and P.M.) using the ROBINS-I tool for non-randomized studies [16]. Discrepancies were resolved by consensus. Risk-of-bias visualization was generated using the ROBVIS tool [17].
Statistical analysis
Meta-analyses were conducted using Review Manager (RevMan version 5.4). Dichotomous variables were pooled using odds ratios (ORs), while continuous outcomes were analyzed using weighted mean differences, both reported with 95% confidence intervals. Statistical heterogeneity was evaluated using the Chi-square test and quantified with the I2 statistic, with values exceeding 50% indicating substantial heterogeneity. Publication bias was assessed through funnel plot analysis and Egger’s regression test.
Results
In the initial database search, 1127 items were found; 163 of them were removed due to duplication. Following abstract screening and the application of the exclusion criteria, 941 of the remaining ones were eliminated. Eighteen were deleted after the entire texts were evaluated to determine their relevance to the review subject. The final evaluation had five papers in total. A PRISMA-style graphic depicting the book selection procedure is shown in Figure 1 [15].
 |
Figure 1 PRISMA: Preferred reporting items for systematic reviews and meta-analyses. |
Five hundred and eighty-five of the five studies used retrograde intramedullary nailing, whereas 894 used antegrade intramedullary nailing [18–22]. The research comprised populations from Sweden, Turkey, Malaysia, Nigeria, and the United States [18–22].
Study characteristics are demonstrated in Table 1 [18–22].
Study characteristics of included studies.
Clinical and radiological findings are summarized in Table 2 [18–22].
Clinical and radiological outcomes (Retrograde vs Antegrade).
Qualitative findings are summarized in Table 3 [18–22].
Qualitative data (Retrograde vs Antegrade).
Refracture after primary operation
According to our research, the antegrade approach had a significantly lower rate of fracture after primary fixation compared to the retrograde approach, with a moderate heterogeneity (OR 31.41; CI – 4.45 – 221.80; p = 0.0.0005; I2 – 28%) as seen in Figure 2.
 |
Figure 2 Demonstrates forrest graph for refracture after primary operation. |
The funnel plot and Egger’s test (p = 0.005), as shown in Figure 3, suggest significant publication bias. A meta-analysis of I2 – 28% shows Moderate heterogeneity.
 |
Figure 3 Demonstrates Funnel plot and Egger’s test for refracture after primary fixation. Predictor – Standard error Z = −2.632, p = 0.008 CI: −5.470 to −0.801. |
Revision
According to our research, the antegrade approach had a significantly lower rate of revision after primary fixation compared to the retrograde approach, with a moderate heterogeneity (OR 1.76; CI – 1.21 – 2.58; p = 0.0.003; I2 – 31%) as seen in Figure 4.
 |
Figure 4 Demonstrates forrest graph for revision after primary fixation. |
The funnel plot and Egger’s test (p = 0.109), as shown in Figure 5, suggest no significant publication bias. A meta-analysis of I2 31% shows Moderate heterogeneity.
 |
Figure 5 Demonstrates Funnel plot and Egger’s test for revision after primary fixation. Predictor – Standard error Z = −1.602, p = 0.109 CI: −0.970 – 0.098. |
Union
According to our research, the antegrade approach had a lower rate of union after primary fixation compared to the retrograde approach (OR 2.06; CI – 0.86 – 4.90; p = 0.10; I2 – 54%) as seen in Figure 6.
 |
Figure 6 Demonstrates forrest graph for union after primary fixation. |
The funnel plot and Egger’s test (p = 0.716), as shown in Figure 7, suggest no significant publication bias. A meta-analysis of I2 – 54% shows Substantial heterogeneity.
 |
Figure 7 Demonstrates Funnel plot and Egger’s test for union after primary fixation. Predictor – Standard error Z = −0.364, p = 0.716 CI: −0.410 – 0.282. |
Malunion
According to our research, the antegrade approach had a higher rate of malunion after primary fixation compared to the retrograde approach (OR 0.85; CI – 0.36 – 2.04; p = 0.72; I2 – N/A) as seen in Figure 8.
 |
Figure 8 Demonstrates forrest graph for malunion after primary fixation. |
The funnel plot and Egger’s test (p = 0.793), as shown in Figure 9, suggest no significant publication bias.
 |
Figure 9 Demonstrates Funnel plot and Egger’s test for malunion after primary fixation. Predictor – Standard error Z = −2.63, p = 0.793 CI: −0.716 – 0.938. |
Delayed union
According to our research, the antegrade approach had a higher rate of delayed union after primary fixation compared to the retrograde approach (OR 0.89; CI – 0.32 – 2.47; p = 0.83; I2 – 64%) as seen in Figure 10.
 |
Figure 10 Demonstrates forrest graph for delayed union after primary fixation. |
The funnel plot and Egger’s test (p = 0.914), as shown in Figure 11, suggest no significant publication bias. A meta-analysis, I2 = 54% shows Substantial heterogeneity.
 |
Figure 11 Demonstrates Funnel plot and Egger’s test for delayed union after primary fixation. Predictor – Standard error Z = 0.108, p = 0.914 CI: −1.510 – 1.687. |
Non-union
According to our research, the antegrade approach had a higher rate of non-union after primary fixation compared to the retrograde approach (OR 0.86; CI – 0.33 – 2.24; p=0.75; I2 – 0%) as seen in Figure 12.
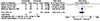 |
Figure 12 Demonstrates forrest graph for non-union after primary fixation. |
The funnel plot and Egger’s test (p = 0.947), as shown in Figure 13, suggest no significant publication bias. A meta-analysis of I2 – 0%.
 |
Figure 13 Demonstrates Funnel plot and Egger’s test for non-union after primary fixation. Predictor – Standard error Z = 0.066, p = 0.947 CI: −0.934 – 0.999. |
Operation time
According to our research, the antegrade approach had similar operative time compared to the retrograde approach (OR 1.48; CI: −3.82 to 6.78; p = 0.58; I2 – 96%) as seen in Figure 14.
 |
Figure 14 Demonstrates forrest graph for mean operative time. |
The funnel plot and Egger’s test (p = 0.869), as shown in Figure 15, suggest no significant publication bias. A meta-analysis of I2 – 96%.
 |
Figure 15 Demonstrates Funnel plot and Egger's test for mean operative time. Predictor. Standard error Z = 0.165, p = 0.869 CI: −1.175 – 1.391. |
Complications
According to our research, the antegrade approach had a lower incidence of complications after primary fixation compared to the retrograde approach (OR 1.10; CI – 0.73 – 1.65; p = 0.65; I2 – 77%) as seen in Figure 16.
 |
Figure 16 Demonstrates forrest graph for complications after primary fixation. |
The funnel plot and Egger’s test (p = 0.742), as shown in Figure 17, suggest no significant publication bias. A meta-analysis of I2 – 77% – shows Considerable heterogeneity.
 |
Figure 17 Demonstrates Funnel plot and Egger’s test for complications after primary fixation. Predictor – Standard error. Z = −0.330, p = 0.742 CI: −1.235 – 0.880. |
Data quality
All of the included studies were either retrospective or prospective studies and were deemed to have a high overall risk of bias due to confounding. Each study included in the meta-analysis is evaluated separately in Figure 18.
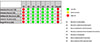 |
Figure 18 ROBINS I ROBVIS tool – Each study included in the meta-analysis is evaluated separately in Figure 18. |
Discussion
With an emphasis on important clinical outcomes such as post-operative fracture healing, revision surgery, nonunion, and malunion, this meta-analysis synthesizes comparative information on antegrade vs retrograde intramedullary nailing (IMN) for femoral shaft and distal femur fractures in older individuals.
Union and nonunion outcomes
Both antegrade and retrograde IMN approaches have shown good overall union rates without statistically significant differences in previous comparative investigations [20]. Retrograde and antegrade nails showed equal healing rates following the index treatment in traditional comparative cohort data, with similar nonunion incidence (about 6% in both groups) and eventual healing following additional surgeries in most patients [20].
Furthermore, when fixation is satisfactory and fracture reduction is adequate, systematic research indicates that nonunion rates are generally modest and not greatly impacted by the direction of nail entrance [23].
Our study reported that retrograde had a higher rate of union than antegrade.
Malunion and alignment
Comparative studies of femoral shaft fractures also show that malunion rates, which indicate the quality of alignment following repair, are generally similar among procedures. In a large retrospective series, for example, malunion was documented in 11% of retrograde and 13% of antegrade instances, with no significant difference between groups [20].
However, compared with retrograde procedures, antegrade nailing may represent a slightly higher risk of loss of coronal alignment in particular fracture subgroups, possibly because of mechanical leverage and entry site biomechanics, according to some data in the larger femoral fracture literature [24].
Our study showed antegrade nailing had a higher rate of malunion and delayed union, though none of our results showed a statistically significant difference.
Revisions and complications
In existing investigations of adult femur fractures, reoperation and revision rates – important indicators of early postoperative failure – do not seem to consistently favor one strategy over the other [25]. The general safety of both procedures for shaft fractures was highlighted by a recent systematic study that compared antegrade and retrograde treatments and found no significant difference in reoperation rates or the majority of secondary problems [25].
Interestingly, the pattern of problems seems to vary depending on the entrance method: anterior knee discomfort is more usually linked to retrograde nailing, while proximal thigh or hip pain is more frequently related to antegrade nailing [20].
Although antegrade intramedullary nailing has been associated with higher rates of malalignment or delayed union in certain fracture patterns, it may paradoxically demonstrate lower revision rates due to several biomechanical and technical factors. Antegrade nails provide a more central, load-sharing construct along the anatomical axis of the femur, which can enhance overall stability and promote sufficient callus formation even in the presence of minor malalignment. In addition, the entry point and proximal fixation allow for better control of femoral length and rotation in many shaft fractures, reducing the likelihood of gross mechanical failure requiring revision. Furthermore, delayed unions following antegrade nailing are often amenable to non-operative management or minor adjuncts (e.g., dynamization), whereas complications associated with alternative techniques may necessitate more complex reoperations [5]. These factors may explain the lower observed revision rates despite theoretical concerns regarding alignment and healing [5].
Our study showed the antegrade approach had a significantly lower rate of revisions and a lower incidence of complications after primary fixation.
Functional outcomes and older patients
Although they are less commonly recorded, functional outcomes in geriatrics that go beyond simple radiographic recovery, such as pain, mobility, and quality of life, are crucial. There are no discernible differences between antegrade and retrograde nails in adult populations according to long-term patient-reported outcomes (such as WOMAC and VAS), indicating that both approaches can produce satisfactory functional recovery [26].
Limitations and implications
The lack of large cohorts specifically targeting older populations (≥65 or ≥80 years) limits the generalisability of existing evidence to the management of geriatric fractures, where physiological reserve, bone quality, comorbidities, and functional demands differ substantially from those of younger cohorts. Many current studies report aggregated outcomes without adequate age stratification, potentially obscuring differences in healing rates, complication profiles, and tolerance to surgical interventions. In older patients, outcomes such as functional recovery, return to independence, mobility, and quality of life are often more clinically meaningful than radiographic union alone. Therefore, future research should prioritize adequately powered, age-stratified analyses and incorporate patient-centered outcome measures, including validated functional scores and health-related quality of life assessments, to better inform decision-making in this growing and high-risk population.
Conclusion
Our study shows that the antegrade approach has lower revision rates despite a higher incidence of malunion and delayed union. The antegrade approach has a lower complication rate, and both approaches have similar operation times. Our authors also suggest an additional advantage of antegrade nailing in elderly patients, as this allows protection of the femoral neck. This study can serve as a basis for further clinical trials in the future.
Funding
Funding is not received for this research.
Conflicts of interest
All authors declare no conflict of interest.
Data availability statement
Data is available upon request.
Author contribution statement
Author 1: Study selection, literature search, data extraction, quality assessment, meta-analysis, writing – original (introduction, methodology, results, and conclusion).
Authors 2, 3, 4, and 5: Study selection, literature search.
Author 6: Meta-analysis, writing – original (results and conclusion).
Author 7: Conceptualization, quality assessment, supervision, and Writing review.
Ethics approval
Ethical approval was not required for this study as it is a systematic review and meta-analysis based exclusively on previously published studies and did not involve direct patient contact or the use of identifiable individual patient data.
Informed consent
The study did not involve individual patient data.
References
- Gwathmey WF, Jones-Quaidoo SM, Kahler D, Hurwitz S, Cui Q (2010) Distal femoral fractures: current concepts. J Am Acad Orthop Surg 18, 597–607. [Google Scholar]
- Martinet O, Cordey J, Harder Y, Maier A, Bühler M, Barraud GE (2000) The epidemiology of fractures of the distal femur. Injury 31, 62–94. [CrossRef] [Google Scholar]
- Gangavalli AK, Nwachuku CO (2016) Management of distal femur fractures in adults. Orthop Clin North Am 47, 85–96. [Google Scholar]
- Tripathy SK, Mishra NP, Varghese P, Panigrahi S, Purudappa PP, Goel A, et al. (2022) Dual-plating in distal femur fracture: a systematic review and limited meta-analysis. Indian J Orthop 56, 183–207. [Google Scholar]
- Ricci WM, Streubel PN, Morshed S, Collinge CA, Nork SE, Gardner MJ (2014) Risk factors for failure of locked plate fixation of distal femur fractures. J Orthop Trauma 28, 83–89. [Google Scholar]
- El-Kawy S, Ansara S, Moftah A, Shalaby H, Varughese V (2007) Retrograde femoral nailing in elderly patients with supracondylar fracture femur. Int Orthop 31, 83–86. [Google Scholar]
- Giddie J, Sawalha S, Parker M (2015) Retrograde nailing for distal femur fractures in the elderly. SICOT J 1, 31. [CrossRef] [EDP Sciences] [PubMed] [Google Scholar]
- Garnavos C, Lygdas P, Lasanianos NG (2012) Retrograde nailing and compression bolts in type C distal femoral fractures. Injury 43, 1170–1175. [Google Scholar]
- Ghandour A, Cosker TDA, Kadambande SS, Pallister I, Russell ID (2006) Experience of the T2 supracondylar nail. Injury 37, 1019–1025. [Google Scholar]
- Aggarwal S, Rajnish RK, Kumar P, Srivastava A, Rathor K, Haq RU (2023) Retrograde nailing versus locking plate fixation: a meta-analysis. J Orthop 36, 36–48. [Google Scholar]
- Smith WR, Ziran BH, Anglen JO, Stahel PF (2007) Locking plates. J Bone Joint Surg Am 89, 2298–2307. [Google Scholar]
- Ricci WM, Loftus T, Cox C, Borrelli J (2006) Locked plates with minimally invasive technique. J Orthop Trauma 20, 190–196. [Google Scholar]
- Wolinsky P, Tejwani N, Richmond JH, Koval KJ, Egol K, Stephen DJG (2002) Intramedullary nailing controversies. Instr Course Lect 51, 291–303. [Google Scholar]
- Fantry AJ, Elia G, Vopat BG, Daniels AH (2015) Distal femoral complications following IM nailing. Orthop Rev (Pavia) 7, 5820. [PubMed] [Google Scholar]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. (2021) PRISMA 2020 statement. BMJ 372, n71. [CrossRef] [Google Scholar]
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. (2019) RoB 2 tool. BMJ 366, l4898. [CrossRef] [PubMed] [Google Scholar]
- McGuinness LA, Higgins JPT (2021) robvis tool. Res Synth Methods 12, 55–61. [Google Scholar]
- Adesina SA, Amole IO, Oyewusi OO, Adefokun IG, Odekhiran EO, Adeniji DO, et al. (2023) Locked IM nailing without fluoroscopy. Int Orthop 47, 1845–1853. [Google Scholar]
- Gönder NÖVKODİH (n.d.) Comparison of femoral fixation methods. The Injector. [Google Scholar]
- Ricci WM, Bellabarba C, Evanoff B, Herscovici D, DiPasquale T, Sanders R (2001) Retrograde versus antegrade nailing. J Orthop Trauma 15, 161–169. [Google Scholar]
- Yu CK, Singh VA, Mariapan S, Chong STB (2007) Antegrade versus retrograde nailing. Eur J Trauma Emerg Surg 33, 135–140. [Google Scholar]
- Bögl HP, Zdolsek G, Michaëlsson K, Höijer J, Schilcher J (2020) Intramedullary nailing outcomes. J Bone Joint Surg Am 102, 1486–1494. [Google Scholar]
- Ma YG, Hu GL, Hu W, Liang F (2016) Nonunion factors in femoral fractures. Chin J Traumatol 19, 109–112. [Google Scholar]
- von Kaeppler EP, Donnelley CA, Roberts HJ, Eliezer EN, Haonga BT, Morshed S, et al. (2021) Retrograde vs antegrade nailing outcomes. OTA Int, 4, e125. [Google Scholar]
- Daher M, Tarchichi J, Zalaquett Z, Casey JC, Ghanimeh J, Mansour J (2024) Antegrade vs retrograde nailing meta-analysis. Arch Bone Jt Surg 12, 535–545. [Google Scholar]
- Brewster J, Grenier G, Taylor BC, Carter C, Degenova D, Ebaugh MP, et al. (2020) Long-term comparison of femoral nailing. Orthopedics 43, e278–e282. [Google Scholar]
Cite this article as: Ravendran K, Khalil MI, Manoharan T, Alexander AA, Shahid N, Abdelghafour K & Mishra P (2026) Comparing outcomes for retrograde intramedullary nailing vs. antegrade intramedullary nailing for Femoral fractures – a systematic review and metaanalysis. SICOT-J 12, 33. https://doi.org/10.1051/sicotj/2026030.
All Tables
All Figures
|
Figure 1 PRISMA: Preferred reporting items for systematic reviews and meta-analyses. |
| In the text | |
|
Figure 2 Demonstrates forrest graph for refracture after primary operation. |
| In the text | |
|
Figure 3 Demonstrates Funnel plot and Egger’s test for refracture after primary fixation. Predictor – Standard error Z = −2.632, p = 0.008 CI: −5.470 to −0.801. |
| In the text | |
|
Figure 4 Demonstrates forrest graph for revision after primary fixation. |
| In the text | |
|
Figure 5 Demonstrates Funnel plot and Egger’s test for revision after primary fixation. Predictor – Standard error Z = −1.602, p = 0.109 CI: −0.970 – 0.098. |
| In the text | |
|
Figure 6 Demonstrates forrest graph for union after primary fixation. |
| In the text | |
|
Figure 7 Demonstrates Funnel plot and Egger’s test for union after primary fixation. Predictor – Standard error Z = −0.364, p = 0.716 CI: −0.410 – 0.282. |
| In the text | |
|
Figure 8 Demonstrates forrest graph for malunion after primary fixation. |
| In the text | |
|
Figure 9 Demonstrates Funnel plot and Egger’s test for malunion after primary fixation. Predictor – Standard error Z = −2.63, p = 0.793 CI: −0.716 – 0.938. |
| In the text | |
|
Figure 10 Demonstrates forrest graph for delayed union after primary fixation. |
| In the text | |
|
Figure 11 Demonstrates Funnel plot and Egger’s test for delayed union after primary fixation. Predictor – Standard error Z = 0.108, p = 0.914 CI: −1.510 – 1.687. |
| In the text | |
|
Figure 12 Demonstrates forrest graph for non-union after primary fixation. |
| In the text | |
|
Figure 13 Demonstrates Funnel plot and Egger’s test for non-union after primary fixation. Predictor – Standard error Z = 0.066, p = 0.947 CI: −0.934 – 0.999. |
| In the text | |
|
Figure 14 Demonstrates forrest graph for mean operative time. |
| In the text | |
|
Figure 15 Demonstrates Funnel plot and Egger's test for mean operative time. Predictor. Standard error Z = 0.165, p = 0.869 CI: −1.175 – 1.391. |
| In the text | |
|
Figure 16 Demonstrates forrest graph for complications after primary fixation. |
| In the text | |
|
Figure 17 Demonstrates Funnel plot and Egger’s test for complications after primary fixation. Predictor – Standard error. Z = −0.330, p = 0.742 CI: −1.235 – 0.880. |
| In the text | |
|
Figure 18 ROBINS I ROBVIS tool – Each study included in the meta-analysis is evaluated separately in Figure 18. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.