| Issue |
SICOT-J
Volume 12, 2026
Special Issue: Newer Horizons in Paediatric Orthopaedics & Trauma
|
|
|---|---|---|
| Article Number | 36 | |
| Number of page(s) | 14 | |
| DOI | https://doi.org/10.1051/sicotj/2026032 | |
| Published online | 05 June 2026 | |
Review Article
Management of pediatric distal radius fractures – A systematic review and meta-analysis
1
Olympia Hospital & Research Centre, 47, 47A Puthur High Road, Puthur, Trichy, Tamilnadu, India
2
Department of Orthopedics, Dhanalakshmi Srinivasan Medical College and Hospital, Perambalur, Tamilnadu, India
3
Department of Orthopaedics, Trichy SRM Medical College, Irungalur, Trichy 621105, Tamilnadu, India
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
22
January
2026
Accepted:
14
April
2026
Abstract
Background: Pediatric distal radius fractures are the most common fractures in children. Management of displaced injuries remains controversial because remodeling capacity varies with skeletal maturity, fracture stability, and fracture subtype. Metaphyseal and physeal fractures differ biologically: metaphyseal injuries are primarily threatened by redisplacement, whereas physeal injuries carry risks of growth disturbance and iatrogenic physeal injury. An evidence-based, maturity- and stability-guided framework is required. Methods: A PRISMA-compliant systematic review and Meta-analysis was performed using PubMed, Embase, Scopus, Web of Science, and the Cochrane Library (inception–2025). Randomized controlled trials and comparative observational studies of pediatric distal radius fractures (0–18 years) treated with cast or splint immobilization, with or without percutaneous Kirschner-wire fixation, were included. Primary outcomes were redisplacement and secondary intervention for metaphyseal fractures; growth disturbance and physeal complications were evaluated separately for physeal injuries. Secondary outcomes included union, functional recovery, complications, and casting quality. Results: Forty-five studies (5,340 patients) were included qualitatively; twelve comparative studies (4 RCTs, 8 observational; 1,455 patients) were analyzed quantitatively (853 cast alone; 602 cast + K-wire). In predominantly metaphyseal fractures, redisplacement occurred in 20–35% after casting versus 0–5% after K-wire fixation (pooled OR 0.10), with reduced secondary intervention (OR 0.15). Union approached 100% and long-term functional outcomes were equivalent. In children with substantial remaining growth, including those <11 years with completely displaced metaphyseal fractures, casting without reduction achieved reliable union and remodeling. For physeal injuries, restoration of physeal alignment and longitudinal growth surveillance were prioritized. Cast length and removable splints demonstrated comparable stability when molding was adequate; casting quality indices were variably predictive. Conclusions: Outcomes are excellent when treatment aligns with fracture biology and skeletal maturity. Metaphyseal and physeal injuries require distinct considerations. Nonoperative care – including acceptance of bayonet apposition in young children – is appropriate for many metaphyseal fractures, while K-wire fixation should be selectively reserved for unstable patterns. Level of evidence: Level II (Systematic review and meta-analysis of Level I–III studies).
Key words: Pediatric distal radius fracture / Cast immobilization / Closed reduction / Kirschner wire fixation / Redisplacement / Fracture remodeling
© The Authors, published by EDP Sciences, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Distal radius fractures are the most common pediatric fractures and a major contributor to emergency visits and fracture-clinic follow-up [1–4]. Despite their frequency, management of displaced fractures remains controversial, with variation in acceptable deformity thresholds, indications for reduction, and use of surgical stabilization [5–9]. Although most minimally displaced fractures heal reliably with immobilization, unstable patterns may redisplace early during casting, leading to remanipulation or delayed fixation [10–15].
Treatment decisions are primarily influenced by two biologic modifiers: (1) skeletal maturity–dependent remodeling potential and (2) fracture stability after reduction. Importantly, metaphyseal and physeal fractures differ in both biology and clinical risk profile. Metaphyseal fractures are principally threatened by redisplacement, whereas physeal injuries carry risks of growth disturbance and iatrogenic physeal injury. Predictors of casting failure in metaphyseal fractures include complete displacement, translation >50%, associated ulnar fracture, residual malalignment, and inadequate cast molding [16–20]. In younger children with substantial remaining growth, even completely displaced metaphyseal fractures may remodel reliably, whereas adolescents have narrower tolerances and reduced remodeling capacity [21–26].
We therefore conducted a systematic review and meta-analysis comparing cast immobilization with and without percutaneous K-wire fixation for displaced pediatric distal radius fractures, integrating fracture subtype, immobilization strategy, cast quality, and skeletal maturity to propose a biologically informed treatment framework.
Materials and methods
Study design
This systematic review and meta-analysis was conducted in accordance with the PRISMA 2020 guidelines and prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD420261290846). Methodological conduct followed the Cochrane Handbook for Systematic Reviews of Interventions.
Literature search
A comprehensive electronic search of PubMed (MEDLINE), Embase, Scopus, Web of Science, and the Cochrane Central Register of Controlled Trials (CENTRAL) was performed from database inception through December 2025. The strategy combined controlled vocabulary (MeSH and Emtree terms) and free-text keywords related to pediatric distal radius fractures, immobilization, closed reduction, Kirschner-wire fixation, redisplacement, and remodeling. Reference lists of eligible studies and relevant conference proceedings (POSNA, AAOS, OTA) were screened manually. No language restrictions were applied.
To address immobilization technique and casting quality, a focused update search was performed using terms related to cast length (short/below-elbow vs long/above-elbow), splinting strategies (removable wrist splints, sugar-tong and double sugar-tong splints), and casting quality indices (cast index, three-point index, gap index). Studies identified through this targeted search were incorporated into the qualitative synthesis and summarized in a dedicated evidence table (Supplementary Tables S1, S2).
Eligibility criteria
Studies were eligible if they included children and adolescents (0–18 years) with distal radius fractures, including metaphyseal and physeal injuries. Studies limited to diaphyseal forearm fractures, pathological fractures, or adult-only populations were excluded unless pediatric distal radius data were separately extractable.
Eligible interventions included cast or splint immobilization, with or without prior closed reduction, and closed reduction followed by percutaneous Kirschner-wire fixation. Alternative fixation strategies, including intrafocal pinning, elastic stable intramedullary nailing, and volar plating, were included in qualitative synthesis but entered quantitative meta-analysis only when a directly comparable cast-versus-K-wire cohort was present.
Because metaphyseal and physeal fractures differ biologically and clinically, fracture subtype was extracted for each study. For metaphyseal fractures, redisplacement and need for secondary intervention were emphasized as primary mechanical outcomes. For physeal injuries, particular attention was given to growth disturbance, physeal complications, and maintenance of symmetric growth. Mixed cohorts without separable data were considered a source of heterogeneity and explored in sensitivity analyses when feasible.
Eligible study designs included randomized controlled trials and comparative cohort studies reporting at least one clinically relevant outcome, including redisplacement, secondary intervention, radiographic alignment, union, functional recovery, complications, or growth disturbance. Case reports, technical notes, biomechanical studies, and small non-comparative series (<30 patients) were excluded.
Study selection and data extraction
Two reviewers independently screened titles and abstracts, followed by full-text assessment using predefined inclusion and exclusion criteria. Disagreements were resolved by consensus; if unresolved, a third reviewer adjudicated. The selection process is illustrated in the PRISMA flow diagram (Figure 1).
 |
Figure 1 PRISMA flow diagram. PRISMA 2020 flow diagram illustrating study identification, screening, eligibility assessment, and inclusion for qualitative synthesis and quantitative meta-analysis. Multiple reports from the same study population were consolidated into single studies for qualitative synthesis. |
Data extraction was performed independently using a standardized form. Extracted variables included study characteristics (design, year, country), patient demographics (age, sex), fracture characteristics (metaphyseal versus physeal, degree of displacement, associated distal ulna fracture), treatment details (reduction method, fixation technique, immobilization strategy), duration of follow-up, and reported outcomes.
Outcomes
The primary outcomes for quantitative synthesis were redisplacement – defined as loss of acceptable alignment on follow-up radiographs – and secondary intervention, defined as repeat reduction or operative fixation following index treatment. Secondary outcomes included fracture union, malunion or residual angulation at final follow-up, functional recovery (range of motion, grip strength, patient-reported outcomes), overall complications, growth disturbance, and refracture. Because radiographic displacement is defined differently by fracture subtype, metaphyseal displacement was extracted as angulation and translation, whereas physeal injuries were extracted using physeal alignment parameters when reported (including widening or gap/step-off of the metaphyseal fragment) and interpreted with priority given to growth-related outcomes.
Risk of bias and certainty of evidence
Randomized controlled trials were evaluated using the Cochrane Risk of Bias 2 (ROB 2) tool. Non-randomized studies were assessed using ROBINS-I and the Methodological Index for Non-Randomized Studies (MINORS). Risk-of-bias assessments informed interpretation but were not used as exclusion criteria. Certainty of evidence for key outcomes was graded using the GRADE framework.
Statistical analysis
Meta-analysis was performed when three or more studies reported comparable outcomes. Dichotomous outcomes were pooled as odds ratios (ORs) with 95% confidence intervals using a random-effects Mantel–Haenszel model, selected a priori to account for anticipated clinical and methodological heterogeneity. Statistical heterogeneity was assessed using the I2 statistic and Cochran’s Q test. A prespecified sensitivity analysis restricted to randomized trials was conducted for primary outcomes. Publication bias was assessed through visual inspection of funnel plots and Egger’s regression test when at least ten studies were available. Statistical significance was defined as p < 0.05.
Data synthesis
Forty-five studies met inclusion criteria for qualitative synthesis. A predefined, non-overlapping subset of twelve comparative studies (four randomized controlled trials and eight observational cohorts), comprising 1,455 pediatric patients, was included in the quantitative meta-analysis.
Study selection and characteristics
Of 3,562 records screened, 45 studies (1994–2025) met criteria for qualitative synthesis (9 randomized controlled trials, 36 observational studies), representing approximately 5,340 pediatric patients (Table 1). Twelve comparative studies (4 RCTs, 8 observational; 1,455 patients) were included in quantitative analysis of cast immobilization alone versus cast plus percutaneous K-wire fixation (853 cast alone; 602 cast + K-wire). Across included studies, mean patient age ranged from 1 to 18 years, with male predominance (60%) (Table 2). Fractures were predominantly metaphyseal (85%); physeal injuries comprised 15%. Associated distal ulna fractures were reported in 70% of cohorts. Open injuries were rare (3%) (Table 3). Physeal injuries were evaluated separately where reported; outcomes extended beyond redisplacement to include growth disturbance and surveillance duration (Figure 2).
Study details.
Overview of included studies and patients.
Fracture characteristics across included studies.
 |
Figure 2 Representative radiographic patterns in pediatric distal radius fractures (AP and lateral views). (a) Torus (buckle) distal radius fracture (stable). (b) Minimally angulated distal metaphyseal fracture. (c) Completely displaced distal metaphyseal fracture. (d) Salter–Harris II distal radius fracture (physeal injury with metaphyseal fragment). |
The quantitative meta-analysis predominantly reflects metaphyseal fracture cohorts; physeal injuries were under-represented in comparative studies and were therefore synthesized qualitatively with emphasis on growth disturbance, physeal complications, and longitudinal surveillance rather than redisplacement.
Immobilization strategy
Cast length
Randomized trials comparing above-elbow versus below-elbow casting demonstrated no significant differences in maintenance of reduction. In a blinded RCT of distal-third forearm fractures, remanipulation criteria were met in 42% (23/55) of above-elbow casts versus 31% (14/45) of below-elbow casts (p = 0.27) [21]. A second RCT similarly found no difference in radiographic stability but reported fewer school absences and improved activities of daily living with short-arm casting [22].
Splints
For minimally angulated metaphyseal fractures not requiring reduction, a randomized trial demonstrated comparable radiographic outcomes between removable splints and short-arm casting; only 6 children (3 per group) required prolonged immobilization, and no surgical interventions occurred [23].
In stable torus fractures (n = 965), an equivalence RCT showed no difference in pain at day 3 (3.21 vs 3.14; adjusted difference − 0.10 within equivalence margin), very low complication rates (1.0% vs 0.6%), and similar school absence (26% vs 22%) [24].
For displaced fractures after reduction, a randomized comparison of double sugar-tong splinting versus long-arm casting demonstrated fewer episodes meeting predefined loss-of-reduction criteria (7 vs 2) and fewer meeting remanipulation thresholds (10 vs 5), with comparable final alignment [25]. A structured sugar-tong protocol maintained reduction in 96% (51/53) of cases [26].
Cast immobilization versus K-wire fixation
Redisplacement
Redisplacement occurred in 20–35% of cast-treated fractures versus 0–5% of K-wire–stabilized fractures (Table 4). Random-effects meta-analysis demonstrated a significant reduction in redisplacement with K-wire fixation (pooled OR 0.10; Figure 3). Effect direction was consistent across study designs.
Distribution of treatment modalities.
 |
Figure 3 Forest plot – redisplacement. Forest plot comparing redisplacement rates between cast immobilization alone and cast immobilization with percutaneous K-wire fixation using a random-effects model. Odds ratios are displayed on a logarithmic scale, with values greater than 1 favoring K-wire fixation. |
Secondary intervention
Repeat reduction or operative stabilization occurred more frequently after casting alone (Figure 4). The pooled estimate significantly favored K-wire fixation (OR 0.15; Table 4). Secondary intervention rates after primary pinning remained low across studies.
 |
Figure 4 Forest plot – Secondary surgery. Forest plot comparing rates of secondary intervention (repeat reduction or surgery) between cast immobilization alone and cast immobilization with K-wire fixation using a random-effects model. Odds ratios are shown on a logarithmic scale. |
Complications
Overall complication rates were low and did not differ significantly between strategies (Figure 5). Cast-related complications were predominantly redisplacement or cast issues; K-wire complications were mainly minor pin-tract infections or migration (Tables 5–6). No consistent signal of long-term morbidity attributable to K-wire fixation was observed.
 |
Figure 5 Forest plot – Complications. Forest plot comparing overall complication rates between cast immobilization alone and cast immobilization with K-wire fixation using a random-effects model. Complications include treatment-related adverse events excluding redisplacement. |
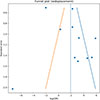 |
Figure 6 Funnel plot – redisplacement. Funnel plot assessing potential publication bias for studies reporting redisplacement outcomes. Visual asymmetry suggests possible small-study effects. |
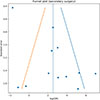 |
Figure 7 Funnel plot – Secondary surgery. Funnel plot evaluating publication bias for secondary surgical intervention outcomes following initial treatment. |
Primary comparative outcomes: cast vs cast + K-wire.
Conservative casting without reduction for overriding fractures (<11 years)
Union and functional outcomes
Union approached 100% regardless of treatment (Table 4). Although early radiographic alignment was more reliably maintained with fixation, long-term wrist motion and functional outcomes were comparable between cast and K-wire groups (Tables 6–8). No study demonstrated superior long-term functional outcomes with routine surgical fixation.
Residual malunion beyond accepted pediatric thresholds was uncommon and rarely symptomatic. When present, remodeling was progressive, particularly in younger children (Table 8).
Overriding (“bayonet”) metaphyseal fractures in children < 11 years
Three comparative studies (n = 180) evaluated completely displaced overriding metaphyseal fractures in children younger than 11 years. Both reduction-based and non-reduction casting strategies achieved 100% union. Acute complications were lower with casting without reduction. Final angulation differences were < 6°, and no functional limitation was reported at follow-up (Table 6).
Surgical technique context
Where reported, K-wire fixation provided the most consistent mechanical stability for unstable displaced fractures. Intrafocal (Kapandji) techniques were described for selected physeal injuries. Elastic intramedullary nailing demonstrated higher implant-related morbidity without clear advantage for distal metaphyseal fractures. Volar plating was primarily reserved for adolescents or intra-articular patterns (Table 7).
Comparison of surgical fixation techniques.
Growth-related outcomes
Growth disturbance was uncommon. Distal radial growth arrest was rare (<2%), ulnar physeal disturbance was usually clinically minor, and refracture rates were low (1–2%) (Table 8).
Long-term outcomes and remodeling.
Publication bias and sensitivity analysis
Funnel plot inspection suggested mild asymmetry for redisplacement and secondary intervention. Egger’s regression indicated possible small-study effects (Figures 5–8). Restriction to randomized trials preserved both direction and magnitude of effect: redisplacement rates ranged from 24–45% after casting versus 0–8% after K-wire fixation [7–9], confirming robustness of pooled findings.
 |
Figure 8 Funnel plot – Complications. Funnel plot assessing publication bias for overall complication outcomes. |
Discussion
This systematic review synthesizes contemporary evidence on pediatric distal radius fracture management and supports a biologically informed, stability-based treatment paradigm rather than routine surgical escalation [1, 2, 10]. Across study designs and patient populations, long-term functional recovery was consistently excellent. The principal clinical challenge is not fracture healing, but prevention of early mechanical failure in unstable patterns [2, 3, 15].
Mechanical stability versus functional outcome
Adjunctive percutaneous K-wire fixation significantly reduces redisplacement and secondary intervention in unstable displaced metaphyseal fractures [7, 8, 10]. In cast-treated cohorts, redisplacement occurs in approximately one-quarter to one-third of cases, whereas primary pin fixation reduces this risk to very low levels [7, 8]. The clinical value of fixation therefore lies in preventing early loss of reduction and repeat procedures.
However, this mechanical advantage does not translate into superior long-term function. Randomized and comparative studies demonstrate equivalent union, wrist motion, and activity levels regardless of fixation [4, 7, 8]. Large contemporary series confirm that K-wires do not eliminate all re-angulation but primarily reduce early instability [16]. Radiographic alignment and patient-centered functional outcome are therefore not synonymous in children, reflecting the remodeling capacity of the distal radius [11, 13, 14].
Immobilization strategy
Immobilization intensity should align with fracture stability. For stable injuries, particularly torus fractures and minimally angulated metaphyseal fractures, removable immobilization is equivalent to casting in functional recovery and fracture stability [23, 24]. These findings are consistent with contemporary guideline recommendations discouraging rigid casting for buckle fractures [27].
Cast length (above-elbow versus below-elbow) does not improve maintenance of reduction when molding is adequate [21, 22]. Stability depends more on fracture characteristics and cast quality than elbow immobilization. For displaced fractures after reduction, sugar-tong–based splinting demonstrates comparable alignment outcomes and low re-intervention rates when applied within structured protocols [25, 26]. These data support graduated immobilization based on fracture stability rather than uniform casting.
Casting quality
Casting failure reflects interaction between intrinsic fracture instability and technique-related factors [28]. Complete displacement, fracture obliquity, and associated ulnar fracture are dominant instability drivers [29]. Casting indices, including the cast index and three-point index, correlate with redisplacement in selected pediatric metaphyseal fractures and function best as adjunctive quality markers rather than standalone thresholds [28, 29]. Their predictive value varies with fracture phenotype and reduction quality. Optimal molding improves stability but does not overcome fundamentally unstable fracture patterns.
Identifying fractures that benefit from fixation
Selective fixation is justified in fractures at high risk of early mechanical failure: complete displacement, translation >50%, associated distal ulna fracture, difficulty maintaining reduction, and limited remaining growth [2, 3, 15]. Age and skeletal maturity are critical modifiers. Remodeling capacity diminishes with advancing maturity, and acceptable deformity thresholds narrow in older children and adolescents [30]. Randomized comparative evidence confirms that unstable fractures in this group frequently fail casting and benefit from primary stabilization [7, 8].
Conversely, evidence supports reconsideration of routine reduction in young children with substantial remaining growth. Completely displaced metaphyseal fractures in children younger than approximately 10–11 years demonstrate reliable union and predictable remodeling even when bayonet apposition is accepted [11]. Early anatomic perfection is therefore not universally required. Chronologic age alone is an imperfect surrogate for remodeling potential. Skeletal maturity occurs earlier in girls than in boys, and treatment decisions should consider remaining growth rather than rigid age cutoffs [30].
Metaphyseal versus physeal injuries
Metaphyseal and physeal distal radius fractures are biologically distinct and carry different clinical priorities. In metaphyseal fractures, the dominant concern is early mechanical failure and redisplacement. In contrast, physeal injuries are defined by the risk of growth disturbance and premature arrest rather than redisplacement alone [5, 31]. Transphyseal fixation introduces a potential iatrogenic threat to the growth plate and must be judiciously weighed against instability [20]. Accordingly, management of physeal injuries prioritizes restoration of physeal alignment and structured longitudinal surveillance to ensure symmetric growth [5, 31]. Displacement metrics also differ by subtype: metaphyseal fractures are characterized by angulation and translation, whereas physeal displacement is more appropriately assessed by physeal alignment and metaphyseal fragment gap or step-off. Treatment algorithms must therefore distinguish these entities rather than apply uniform radiographic thresholds.
Complications and surgical context
Overall complication rates were low across treatment strategies [7, 8]. Cast-related complications primarily reflected mechanical failure, whereas K-wire complications were typically minor and self-limited [6, 16]. More invasive alternatives – including elastic intramedullary nailing and plating – carry greater implant-related morbidity and should be reserved for specific indications such as irreducible, intra-articular, or near-mature fractures [10, 30].
Proposed framework
The proposed algorithm integrates fracture stability, skeletal maturity, and fracture subtype. Where high-quality comparative evidence exists, recommendations are direct; elsewhere, guidance reflects synthesis of best available data and established principles of pediatric fracture biology (Figure 9).
 |
Figure 9 Evidence-based treatment framework for pediatric distal radius fractures. The algorithm categorizes management based on fracture biology (metaphyseal vs. physeal) and mechanical stability. Metaphyseal Pathway: Focuses on graduated immobilization. Stable injuries (e.g., Torus) are managed with minimal intervention. Displaced but stable injuries receive closed reduction and molded casting. Fixation is selectively reserved for “High Risk” patterns to prevent early redisplacement. In children under 11 years, bayonet apposition is often acceptable due to high remodeling potential. Physeal Pathway: Prioritizes growth plate preservation. For unstable SH II injuries, intrafocal (Kapandji) K-wire pinning provides rigid fixation while strictly avoiding transphyseal iatrogenic injury. Note: Chronological age thresholds are clinical proxies; treatment decisions must be adjusted based on individual growth velocity and sex-specific maturity. |
Limitations
Clinical heterogeneity in fracture definitions, immobilization techniques, and redisplacement thresholds limits precision of pooled estimates. Observational comparisons introduce potential confounding by indication, although consistency of effect across randomized trials mitigates this concern [7, 8]. Functional outcomes were inconsistently reported, and cost-effectiveness data remain limited. Funnel plot asymmetry suggests possible small-study effects; however, effect direction remained stable in sensitivity analyses [10].
Conclusions
Pediatric distal radius fractures demonstrate predictable healing and excellent long-term function when treatment is aligned with fracture biology and skeletal maturity rather than radiographic perfection alone. Metaphyseal and physeal injuries require distinct consideration: metaphyseal fractures are primarily threatened by early mechanical instability, whereas physeal injuries demand vigilance for growth disturbance and symmetric remodeling.
Nonoperative management remains appropriate for the majority of fractures, including acceptance of bayonet apposition in children with substantial remaining growth. Removable splints, short-arm casting, and graduated immobilization strategies are safe and effective for stable patterns. Percutaneous K-wire fixation should be reserved for fractures at high risk of early failure – particularly unstable displaced patterns in older children and adolescents with diminishing remodeling capacity – where its principal benefit lies in preventing redisplacement and secondary intervention, not in improving ultimate functional outcome.
The Ccentral message of this review is clear: stability and skeletal maturity – not uniform radiographic thresholds – should guide management. A selective, maturity- and stability-based strategy minimizes unnecessary intervention while preserving the excellent natural history of pediatric distal radius fractures.
Acknowledgments
Declaration of generative AI and AI-assisted technologies in the writing process: During preparation of this manuscript, the authors used ChatGPT 5 for language refinement and readability. The tool was not used to generate scientific content, data, or interpret results. All output was reviewed and edited by the authors, who take full responsibility for the accuracy and integrity of the manuscript.
Funding
No funding was received for this study.
Conflicts of interest
The authors declare that they have no conflicts of interest related to this work.
Data availability statement
All data generated or analyzed during this study are included in this published article.
Ethics approval
This study is based on a review of previously published literature and did not involve new studies with human participants or animals; therefore, formal ethics approval was not required.
Author contribution statement
J Terrence Jose Jerome: Conceptualization, Data curation, Writing – original draft.
G Surendran: Methodology, Data curation, Writing – review & editing.
Thirumagal Kuppusamy: Visualization, Validation, Writing – review & editing.
Supplementary material
Table S1: Randomized control trials and other evidence base studies. Access Supplementary Material
Table S2: Technique-focused series and noncomparative cohorts included in qualitative synthesis (not pooled in meta-analysis). Access Supplementary Material
References
- Labianca L, Calderaro C, Maffulli N (2024) Pediatric wrist fractures: variations in management across countries. Br Med Bull 152, 1, 28–34. [Google Scholar]
- Rai P, Haque A, Abraham A (2020) A systematic review of displaced paediatric distal radius fracture management: plaster cast versus Kirschner wiring. J Clin Orthop Trauma 11, 275–280. [Google Scholar]
- Constantino DMC, Machado L, Carvalho M, et al. (2021) Redisplacement of paediatric distal radius fractures: what is the problem? J Child Orthop 15, 532–539. [Google Scholar]
- Wendling-Keim DS, Wieser B, Dietz HG (2015) Closed reduction and immobilization of displaced distal radial fractures. Eur J Trauma Emerg Surg 41, 421–428. [Google Scholar]
- Ward CM, Larsen MC, Bohm KC, Rizkala AR (2016) Outcomes of nonoperative treatment of Salter-Harris II distal radius fractures: a systematic review. HAND 11, 1, 29–35. [Google Scholar]
- Ozcan M, Memisoglu S, Copuroglu C, Saridogan K (2010) Percutaneous Kirschner wire fixation in distal radius metaphyseal fractures in children: does it change the overall outcome? Hippokratia 14 (4), 265–270. [Google Scholar]
- Miller BS, Taylor B, Widmann RF, Bae DS, Snyder BD, Waters PM (2005) Cast immobilization versus percutaneous pin fixation of displaced distal radius fractures in children: a prospective randomized study. J Pediatr Orthop 25(4), 490–494. [Google Scholar]
- McLauchlan GJ, Cowan B, Annan IH, Robb JE (2002) Management of completely displaced metaphyseal fractures of the distal radius in children: a prospective randomized controlled trial. J Bone Joint Surg Br 84, 413–417. [Google Scholar]
- Colaris JW, Allema JH, Biter LU, de Vries MR, van de Ven CP, Bloem RM, Kerver AJ, Reijman M, Verhaar JA (2013) Re-displacement of stable distal both-bone forearm fractures in children: a randomized controlled multicentre trial. Injury 44, 498–503. [Google Scholar]
- Alotaibi MN, Aldaraani LGA, Altala AS, et al. (2025) Comparing the outcomes of cast immobilization with and without K-wire fixation for displaced distal radius fractures in the pediatric population: a systematic review and meta-analysis. Medicina (Kaunas) 61 (5), 852. [Google Scholar]
- Galán-Olleros M, Mayans-Sanesteban J, Martínez-Álvarez S, et al. (2024) Is reduction necessary in overriding metaphyseal distal radius fractures in children under 11 years: a systematic review and meta-analysis. Eur J Orthop Surg Traumatol 34, 5, 2225–2234. [Google Scholar]
- Vescio A, Testa G, Montemagno M, Sapienza M, Pavone V (2021) Secondary displacement risk after reduction and cast immobilization of displaced distal radius fractures in overweight and obese children: a systematic review and meta-analysis. Miner Orthop 72 (1), 71–76. [Google Scholar]
- Pannu GS, Herman M (2015) Distal radius-ulna fractures in children. Orthop Clin North Am 46, 235–248. [Google Scholar]
- Bae DS (2008) Pediatric distal radius and forearm fractures. J Hand Surg Am 33 (10), 1911–1923. [Google Scholar]
- Nietosvaara Y, Hasler C, Helenius I, Cundy P (2005) Marked initial displacement predicts complications in physeal fractures of the distal radius: an analysis of fracture characteristics, primary treatment and complications in 109 patients. Acta Orthop 76 (6), 873–877. [Google Scholar]
- Ramoutar DN, Shivji FS, Rodrigues JN, Hunter JB (2015) Outcomes of displaced paediatric distal radius fractures treated with percutaneous Kirschner wire fixation: a review of 248 cases. Eur J Orthop Surg Traumatol 25, 471–476. [Google Scholar]
- Satish BRJ, Vinodkumar M, Suresh M, Seetharam PY, Jaikumar K (2014) Closed reduction and K-wiring with the Kapandji technique for completely displaced pediatric distal radial fractures. Orthopedics 37 (9), e810–e816. [Google Scholar]
- Valisena S, Gonzalez JG, Voumard NM, et al. (2019) Treatment of paediatric unstable displaced distal radius fractures using Kapandji technique: a case series. Eur J Orthop Surg Traumatol 29, 413–420. [Google Scholar]
- Bassi C, Heimann AF, Schwab JM, Tannast M, Raabe I (2024) Modified Kapandji technique in pediatric displaced distal radius fractures: results in 195 patients. Eur J Orthop Surg Traumatol 34, 489–497. [Google Scholar]
- Jerome JTJ (2021) Salter-Harris II distal radial fractures treated with the intrafocal K-wire technique: a retrospective study of 20 cases. J Hand Surg Eur 46 (5), 471–475. [Google Scholar]
- Bohm ER, Bubbar V, Yong Hing K, Dzus A (2006) Above and below-the-elbow plaster casts for distal forearm fractures in children. A randomized controlled trial. J Bone Joint Surg Am 88(1), 1–8. [Google Scholar]
- Webb GR, Galpin RD, Armstrong DG (2006) Comparison of short and long arm plaster casts for displaced fractures in the distal third of the forearm in children. J Bone Joint Surg Am 88(1), 9–17. [Google Scholar]
- Boutis K, Willan A, Babyn P, Goeree R, Howard A (2010) Cast versus splint in children with minimally angulated fractures of the distal radius: a randomized controlled trial. CMAJ 182(14), 1507–12. [Google Scholar]
- Perry DC, Achten J, Knight R, Appelbe D, Dutton SJ, Dritsaki M, Mason JM, Roland DT, Messahel S, Widnall J, Costa ML, FORCE Collaborators in collaboration with PERUKI (2022) Immobilisation of torus fractures of the wrist in children (FORCE): a randomised controlled equivalence trial in the UK. Lancet 400(10345, 39–47. Erratum in: Lancet. 2022 Jul 23;400(10348):272. https://doi.org/10.1016/S0140-6736(22)01342-3. Erratum in: Lancet. 2022 Oct 1;400(10358):1102. https://doi.org/10.1016/S0140-6736(22)01734-2. PMID: 35780790 . [Google Scholar]
- Levy J, Ernat J, Song D, Cook JB, Judd D, Shaha S (2015) Outcomes of long-arm casting versus double-sugar-tong splinting of acute pediatric distal forearm fractures. J Pediatr Orthop 35(1), 11–17. [Google Scholar]
- Denes AE Jr, Goding R, Tamborlane J, Schwartz E (2007) Maintenance of reduction of pediatric distal radius fractures with a sugar-tong splint. Am J Orthop (Belle Mead NJ). 36(2), 68–70. [Google Scholar]
- Ali F, Elmubark M, Mussab RM, Mubark I, Jayakumar N, Ashwood N (2024) Improving Patient care and streamlining follow-up: compliance with national institute for health and care excellence (NICE) guidelines for pediatric distal radius buckle fractures. Cureus 16(11), e73624. [Google Scholar]
- Pretell Mazzini J, Rodriguez Martin J (2010) Paediatric forearm and distal radius fractures: risk factors and re-displacement--role of casting indices. Int Orthop. 34(3), 407–412. [Google Scholar]
- Alemdaroğlu KB, Iltar S, Cimen O, Uysal M, Alagöz E, Atlihan D (2008) Risk factors in redisplacement of distal radial fractures in children. J Bone Joint Surg Am 90(6), 1224–1230. [Google Scholar]
- Greig D, Silva M (2021) Management of distal radius fractures in adolescent patients. J Pediatr Orthop 41(Suppl 1), S1–S5. [Google Scholar]
- Bellaire LL, Vuillermin C, Vuillermin C, et al. (2021) Traumatic physeal arrests at the wrist. J Ped Orthop Soc N Am 3(2), 265. [Google Scholar]
Cite this article as: : Jerome JTJ, Surendran G & Kuppusamy T (2026) Management of pediatric distal radius fractures – A systematic review and meta-analysis. SICOT-J 12, 36. https://doi.org/10.1051/sicotj/2026032.
All Tables
All Figures
|
Figure 1 PRISMA flow diagram. PRISMA 2020 flow diagram illustrating study identification, screening, eligibility assessment, and inclusion for qualitative synthesis and quantitative meta-analysis. Multiple reports from the same study population were consolidated into single studies for qualitative synthesis. |
| In the text | |
|
Figure 2 Representative radiographic patterns in pediatric distal radius fractures (AP and lateral views). (a) Torus (buckle) distal radius fracture (stable). (b) Minimally angulated distal metaphyseal fracture. (c) Completely displaced distal metaphyseal fracture. (d) Salter–Harris II distal radius fracture (physeal injury with metaphyseal fragment). |
| In the text | |
|
Figure 3 Forest plot – redisplacement. Forest plot comparing redisplacement rates between cast immobilization alone and cast immobilization with percutaneous K-wire fixation using a random-effects model. Odds ratios are displayed on a logarithmic scale, with values greater than 1 favoring K-wire fixation. |
| In the text | |
|
Figure 4 Forest plot – Secondary surgery. Forest plot comparing rates of secondary intervention (repeat reduction or surgery) between cast immobilization alone and cast immobilization with K-wire fixation using a random-effects model. Odds ratios are shown on a logarithmic scale. |
| In the text | |
|
Figure 5 Forest plot – Complications. Forest plot comparing overall complication rates between cast immobilization alone and cast immobilization with K-wire fixation using a random-effects model. Complications include treatment-related adverse events excluding redisplacement. |
| In the text | |
|
Figure 6 Funnel plot – redisplacement. Funnel plot assessing potential publication bias for studies reporting redisplacement outcomes. Visual asymmetry suggests possible small-study effects. |
| In the text | |
|
Figure 7 Funnel plot – Secondary surgery. Funnel plot evaluating publication bias for secondary surgical intervention outcomes following initial treatment. |
| In the text | |
|
Figure 8 Funnel plot – Complications. Funnel plot assessing publication bias for overall complication outcomes. |
| In the text | |
|
Figure 9 Evidence-based treatment framework for pediatric distal radius fractures. The algorithm categorizes management based on fracture biology (metaphyseal vs. physeal) and mechanical stability. Metaphyseal Pathway: Focuses on graduated immobilization. Stable injuries (e.g., Torus) are managed with minimal intervention. Displaced but stable injuries receive closed reduction and molded casting. Fixation is selectively reserved for “High Risk” patterns to prevent early redisplacement. In children under 11 years, bayonet apposition is often acceptable due to high remodeling potential. Physeal Pathway: Prioritizes growth plate preservation. For unstable SH II injuries, intrafocal (Kapandji) K-wire pinning provides rigid fixation while strictly avoiding transphyseal iatrogenic injury. Note: Chronological age thresholds are clinical proxies; treatment decisions must be adjusted based on individual growth velocity and sex-specific maturity. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.