| Issue |
SICOT-J
Volume 12, 2026
|
|
|---|---|---|
| Article Number | 30 | |
| Number of page(s) | 7 | |
| Section | Knee | |
| DOI | https://doi.org/10.1051/sicotj/2026003 | |
| Published online | 19 May 2026 | |
Original Article
Tibial tunnel malposition is a risk factor for osteoarthritis following ACL reconstruction at long term follow up: a retrospective study
1
Univ Lyon, Claude Bernard Lyon 1 University, IFSTTAR, LBMC UMR_T9406, F-69622, Lyon, France
2
Orthopaedics surgery and Sports Medicine Department, FIFA medical center of excellence, Croix-Rousse Hospital, Lyon University Hospital, Lyon, France
3
Ortopedia e Traumatologia, Fondazione Poliambulanza Istituto Ospedaliero, Brescia, Italy
4
LIBM – EA 7424, Interuniversity Laboratory of Biology of Mobility, Claude Bernard Lyon 1 University, Lyon, France
* Corresponding Author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
17
November
2025
Accepted:
26
January
2026
Abstract
Purpose: This study aimed to compare long-term radiographic OA development after ACLR according to tunnel positioning assessed on 3D postoperative CT scans. Methods: Tunnel positioning was studied using 3D reconstructions, and tunnels were considered malpositioned if femoral tunnels were classified as type II or III (F), and tibial tunnels had an anteroposterior (AP) gap ≥ 5 mm and/or a mediolateral (ML) gap ≥ 2 mm compared to the native ACL location. Advanced radiographic OA was stages C and D according to the IKDC classification. Results: In this retrospective study, 76 consecutive patients who underwent ACLR were evaluated at a mean follow-up of 10.4 years. The mean age was 34.0 years. At the last follow-up, 18.4% of the patients had an advanced radiographic stage of OA. The distribution of malpositioned tunnels was as follows: 30.3% F, 17.1% AP, 19.7% ML, 11.8% AP+ML, and 5.3% AP+ML+F. There was a significant association between AP+ML (p = 0.022) and AP+ML+F (p < 0.001) tunnels and the IKDC C/D group. Conclusion: The malpositioning of tibial tunnels, specifically the combination of ML and AP displacement, is significantly associated with an advanced radiographic stage of OA at a follow-up of 10 years, regardless of femoral tunnel malposition. Level of Evidence: Level II.
Key words: Tunnel position / CT-scan / ACL reconstruction / Osteoarthritis / Anterior cruciate ligament
© The Authors, published by EDP Sciences, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Anterior cruciate ligament (ACL) injury is a common orthopaedic injury. Incidence ranges between 60.9 and 78 per 100 000 person-years in the literature [1, 2]. This injury has significant implications, including post-traumatic osteoarthritis (OA) [3]. An anatomical ACL reconstruction (ACLR) with optimal tunnel positioning is essential to restore the knee’s native kinematics [4]. After ACL injury, irrespective of whether the patients were treated operatively or nonoperatively, the relative risk of developing OA increased [5]. Despite the significant number of ACLRs carried out each year, technical errors remain frequent and play a contributing role in failures [6]. The transtibial femoral tunnel positioning technique is less accurate [7] and has been associated with higher rates of OA at longterm follow up compared with the antero-medial approach for femoral tunnel positioning [8]. Tunnel malposition is one of the leading causes of technical errors and is widely observed among the reasons for ACL revisions [9]. Historically and in daily practice, radiography is widely used to analyze tunnel positioning. However, some authors highlight the lack of precision of these techniques [10]. Recently, several protocols using cross-sectional imaging have been described, allowing precise identification of bony landmarks and ACL footprints [11].
Previous studies reported an association between sagittal tibial tunnel position and radiographic OA [12], whereas others found no correlation [13]. Regarding femoral tunnel placement, previous studies also shown conflicting results [14, 15]. None of the studies evaluating long-term OA after ACL reconstruction used 3D reconstructions from postoperative CT scan to classify tunnel positioning.
The aim of this study was to compare long-term radiological development of OA after ACLR according to tunnel positioning, identified on 3D reconstructions from postoperative CT scan. The hypothesis was that a higher rate of radiological OA was associated with non-anatomical tunnel positioning at long- term follow-up.
Methods
Patients
Consecutive patients aged between 15 and 60 years old from a single institution undergoing primary ACLR between February 2012 and December 2015 were included in this retrospective study. Patients underwent arthroscopic ACLR using a single-bundle technique with an outside-in drilling technique in all cases. First, a diagnostic arthroscopy was performed, followed by a systematic assessment of the cartilage and menisci. Meniscus repair was performed whenever possible. Meniscal resection was only performed for vertical flap and radial tears in zone 3, complex lesions with degenerative tissue, or failed repairs. All data were collected retrospectively from the medical records.
As part of the standard practice of the department during this time period, CT scans were obtained within 6 weeks postoperatively to evaluate tibial and femoral tunnel positioning. Each CT scan was performed by the same imaging service. The scanner was a CR-Brilliance CT (cut thickness, 0.67 mm; increment, 0.33 mm). The images were processed using Centricity® software (GE Medical Systems, Chicago, IL; 2006).
The evaluation of ACL tear was conducted clinically using the Lachman test and pivot shift test, with confirmation provided by an MRI. Exclusion criteria were patients with preoperative radiographic OA (IKDC stage B, C, or D) [16].
One patient was excluded for preoperative advanced OA on radiography. A total of 76 ACLRs were included in the study group with a mean follow-up of 10.4 years (IQR 9.9–11.1). Mean age at surgery was 34.0 years (IQR 24.1–46.5) with an average BMI of 23.2 kg/m2 (IQR 21.1–25.8). Grafts consisted of either BPTB (70; 92.1%), 4-strand HT (5; 6.6%), or QT (1; 1.3%). Medial or lateral menisectomy was performed for 18 (23.7%) patients. The presence of a cartilage lesion was described for 6 (7.9%) patients. Patient characteristics are summarized in Table 1.
Cohort characteristics.
Tibial tunnel position
Intra-articular tibial tunnel position was analyzed using the intercondylar area method described by Cremer et al. [17] (Figure 1).
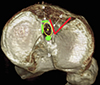 |
Figure 1 3-D CT scan reconstruction of a right tibial plateau axial view. Bony landmarks for ACL footprint and its center (yellow circle and yellow dot) are represented (a, anterior ridge; b, intertubercular fossae; c, medial intercondylar ridge; d, medial border of the lateral groove). |
 |
Figure 2 3-D rCT scan reconstructed images allow assessment of the intra-articular femoral tunnel aperture. a. Distal view. b. Medial view. c. Posterior view. d. Posteromedial view. |
Tibial tunnel aperture was considered malpositioned if the anteroposterior (AP) gap between the center of the tunnel and the center of the ACL footprint was ≥ 5 mm or the mediolateral (ML) gap between the center of the tunnel and the center of the ACL footprint was ≥ 2 mm.
Femoral tunnel position
Four 3-D reconstructed images were provided to allow assessment of the intra-articular femoral tunnel aperture (Figure 2). Intra-articular femoral tunnel position was analyzed using the technique described by Magnussen et al. [18]. The classification system is based on the location of the femoral tunnel relative to the lateral intercondylar ridge, with the knee flexed at 90° as during arthroscopy (Figure 3). The femoral tunnel was classified as type I, or anatomical, if it was located entirely below and posterior to the lateral intercondylar ridge as viewed from distally. The tunnel was classified as type II, or intermediate, if it was slightly malpositioned vertically, anteriorly, or both, such that the tunnel overlapped the lateral intercondylar ridge. The tunnel was classified as type III, or non-anatomical, if it was significantly malpositioned and located entirely anterior and/or vertical to the lateral intercondylar ridge. Tunnels type II and III (F) were considered malpositioned.
 |
Figure 3 3-D CT scan reconstruction of the right distal femur illustrating the femoral tunnel classification system for the anterior cruciate ligament (ACL). a. Distal view. b. Medial view. c. Posterior view. d. Posteromedial view. Type I tunnels (appropriately positioned or anatomical) are entirely contained within the green zone, located posterior and inferior to the lateral intercondylar ridge (black line). Type II tunnels (slightly malpositioned) partially overlap the lateral intercondylar ridge and extend into the orange zone. Type III tunnels (severely malpositioned or non-anatomical) are positioned completely anterior and superior to the lateral intercondylar ridge, extending into the red zone. |
Osteoarthritis and prognostic factors
Weight-bearing antero-posterior, schuss and lateral radiographs were obtained and assessed before the surgery and at the last follow-up for signs of OA according to the International Knee Documentation Committee (IKDC) classification [16]. Stages C and D indicating advanced stage of OA. Age at surgery, sex, injury-to-surgery time, body mass index (BMI), meniscectomy, type of sport, and cartilaginous status were also assessed.
Ethical approval
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee, the 1964 Helsinki declaration and its later amendments, or comparable ethical standards. Data collection and analysis were carried out in accordance with MR004 Reference Methodology (Ref. 2238218v0) obtained on March 24, 2025. The study was registered and filed on the Health Data Hub website.
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD) or as median and IQR, while categorical variables were presented as frequency distributions and percentages. The Shapiro–Wilk test was employed to evaluate the normality of the data. For comparisons between two groups, either the t-test or the Mann–Whitney U test was used, depending on whether the data followed a normal distribution. Categorical variables were analyzed using the chi-square test.
Finally, a multivariate analysis was carried out using a logistic regression model in order to calculate the Odds Ratio (OR) and its confidence intervals. A 95% confidence interval was applied, and statistical significance was defined as a p-value < 0.05.
All statistical analyses were performed using Python version 3.11 (Python Software Foundation, Wilmington, DE, USA) and the stats models library (v0.13).
Results
Femoral tunnel position
Of the 76 ACLRs performed, 53 (69,7%) were well-positioned, 17 (22.4%) were slightly malpositioned (overlapping the resident’s ridge), and 6 (7.9%) were significantly malpositioned (entirely vertical and/or anterior to the resident ridge). As such, 23 tunnels were considered malpositioned (30%) (type II and type III) (Table 2a).
a. Distribution of femoral tunnel position. b. Distribution of tibial tunnel position
Tibial tunnel position
Of the study group, 13 patients (17%) had an AP gap ≥ 5 mm and 15 (19%) a ML gap ≥ 2 mm. Association of AP and ML malposition was observed for 9 patients (11%). Global tunnels malposition (AP + ML + F) occurred for 4 patients (5%) (Table 2b).
Osteoarthritis
The radiographs showed evidence of an advanced stage of OA in 18% of cases. At last follow-up, 60.5% of patients were IKDC A, 21.1% IKDC B, 10.5% IKDC C, and 7.9% IKDC D.
Global tunnel positions depending on the IKDC radiographic grade of OA are presented in Table 3.
Tunnel positions depend on IKDC radiographic stage of OA.
Significant association between AP+ML and AP+ML+F tunnels and the IKDC C/D group (p = 0.022 and p < 0.001, respectively) was found.
Prognostic factors
The performance of a meniscectomy and the presence of cartilage lesions were significantly associated with an advanced radiographic stage of OA (p < 0.001 and p = 0.008, respectively). Distribution of independent risk factors is summarized in Table 4.
Distribution of independent risk factors for osteoarthritis.
Discussion
The main finding of this study was that a non-anatomic position of the tibial tunnel and the combined malposition of both the tibial and femoral tunnels were associated with long-term radiographic OA. Isolated non-anatomic positioning of the femoral tunnel was not associated with OA in this study.
This study has some limitations. First, it has a retrospective design and a limited number of patients. Additionally, radiographs of the contralateral healthy limb were not available to compare the radiographic stage of OA, nor were long-leg films obtained to assess any pre-existing lower limb deformities. Cartilage lesions and the performance of concomitant meniscectomy were recorded as either present or absent, without grading severity or specifying compartmental location.
In this study, the 3D CT-scan tool was used to evaluate the positioning of the tunnels after ACLR. In 2005, Hoser et al. demonstrated that the 3D scanner was a reliable method in routine practice, compared to conventional radiographs, which showed low reliability (p = 0.22) [19].
Concerning tibial tunnels, 48% of the patients had non anatomic position in this study. This result can be explained by the complexity and variation of the footprint in itself. Pedneault et al., in their study on 40 patients, observed that the reconstructed tibial footprint was placed too anteriorly and medial to the ACL native footprint, while Shi et al. found that the average tunnel position was too lateral at the tibial side [14, 20]. Pedneault et al. found that the mean distance between the center of the native and reconstructed ACL at the tibial attachment site was 6.24 mm, and more than half the patients had less than 50% overlap with the native footprint [14]. The link between tibial tunnel malposition and OA can be explained by biomechanics. Anterior tibial tunnel placement significantly reduced anterior tibial translation and pivot shift movement, but may result in a roof impingement associated with a loss of extension and abrasion of the replacement graft, while excessively posterior tibial tunnel positioning fails to control laxity [15]. Contrary to anteroposterior graft placement, coronal tunnel location seems to have minimal effect on knee biomechanics [21]. The influence of sagittal positioning on the development of OA is discussed in the literature. Jin Hwan Ahn et al. highlighted in a 10-year mean follow-up study the importance of the sagittal tunnel position on the medial femoro-tibial compartment, while de Mees et al. found that tibial tunnel positions were not associated with radiographic OA [12, 13].
Concerning the femoral tunnel, approximatively 30% of them were considered as malpositioned in this study. In the literature, femoral tunnel placement appears to be a major key point for anatomic ACLR. Morgan et al. found that femoral tunnel malposition was cited in 219 (47.6%) of 460 revision cases [22]. Seo et al. found that 30% of femoral tunnel placement was too anterior, resulting in excessive residual laxity [23]. Shi et al. found that, at the femoral side, the average tunnel position in the ACLR failure group was significantly more anterior and superior [20]. Moreover, the specific risk of meniscal surgery after ACLR appears to be increased after femoral tunnel malposition [24]. In this study, isolated femoral tunnel malpositioning was not associated with an advanced stage of OA. This result is consistent with studies with a long-term follow-up [14]. It can be explained by the low number of type III tunnels (7.9%) and the technique used to perform femoral tunnels. Osti et al. showed that anteromedial portal and outside-in surgical techniques were superior in positioning the ACL femoral tunnel at the center of the native ACL attachment site compared with the transtibial technique [15].
In this study, the advanced stage of OA was found in 18% of cases, which is similar to studies with the same follow-up [14]. Associated injuries, especially medial and lateral meniscectomy and cartilage lesions, play a major role in OA in this study, which has also been widely found in the literature [25].
Conclusion
The malpositioning of tibial tunnels, specifically the combination of ML and AP displacement, is significantly associated with an advanced radiographic stage of OA at a follow-up of ten years, regardless of femoral tunnel malposition.
Additionally, undergoing a meniscectomy or identifying a cartilage lesion during ACLR has been identified as a risk factor for an advanced radiographic stage of OA at a follow-up of ten years.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interest
JE, MR, LA, CB: declare that they have no conflict of interest.
ES: Paid presentations from Smith Nephew.
SL: Royalties from Stryker, Smith and Nephew, and consultancy for Heraeus, Depuy Synthes, and Serf. Institutional research support from Groupe Lepine and Amplitude. Editorial Board for Journal of Bone and Joint Surgery (Am).
Data availability statement
The data that support the findings of this study are not openly available due to reasons of sensitivity and are available from the corresponding author upon reasonable request.
Author contribution statement
JE: study design, statistical analysis, literature review, and manuscript writing; MR: data collection, statistical analysis, literature review, and manuscript writing; LA: literature review and manuscript editing; CB: study design, statistical analysis, literature review, and manuscript editing; SL: study design, supervision, literature review, and manuscript editing; ES: study design, supervision, literature review, and manuscript editing.
Ethics approval
All procedures were performed in accordance with the ethical standards of the institutional and/or national research committee, the 1964 Helsinki declaration and its later amendments, or comparable ethical standards. Data collection and analysis were carried out in accordance with MR004 Reference Methodology (Ref. 2238218v0) obtained on March 24, 2025. The study was registered and filed on the Health Data Hub website. Declaration of Generative AI and AI-assisted technologies in the writing process. No AI was used for the writing of the submitted work. All authors read and approved the final manuscript.
References
- Erard J, Cance N, Shatrov J, et al. (2023) Delaying ACL reconstruction is associated with increased rates of medial meniscal tear. Knee Surg Sports Traumatol Arthrosc 31, 4458–4466. [Google Scholar]
- Mesnard G, Fournier G, Joseph L, et al. (2022) Does meniscal repair impact muscle strength following ACL reconstruction?. SICOT J 8, 16. [Google Scholar]
- Cance N, Erard J, Shatrov J, et al. (2023) Delaying anterior cruciate ligament reconstruction increases the rate and severity of medial chondral injuries. Bone Joint J 105-B, 953–960. [Google Scholar]
- Fox MA, Zsidai B, Dadoo S, et al. (2023) Anatomic anterior cruciate ligament reconstruction. Arthroscopy 39, 1968–1970. [Google Scholar]
- Ajuied A, Wong F, SmithC, et al. (2014) Anterior cruciate ligament injury and radiologic progression of knee osteoarthritis: a systematic review and meta-analysis. Am J Sports Med 42, 2242–2252. [Google Scholar]
- Di Benedetto P, Di Benedetto E, Fiocchi A, et al. (2016) Causes of failure of anterior cruciate ligament reconstruction and revision surgical strategies. Knee Surg Relat Res 28, 319–324. [Google Scholar]
- Mastrokalos D, Roustemis AG, Koulalis D (2025) Limited accuracy of transtibial aiming for anatomical femoral tunnel positioning in ACL reconstruction. SICOT J, 11, 8. [Google Scholar]
- Cinque ME, Kunze KN, Williams BT, et al. (2022) Higher incidence of radiographic posttraumatic osteoarthritis with transtibial femoral tunnel positioning compared with anteromedial femoral tunnel positioning during anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med 50, 255–263. [Google Scholar]
- Byrne KJ, Hughes JD, Gibbs C, et al. (2022) Non-anatomic tunnel position increases the risk of revision anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc 30, 1388–1395. [Google Scholar]
- Luites JWH, Verdonschot N (2017) Radiographic positions of femoral ACL, AM and PL centres: accuracy of guidelines based on the lateral quadrant method. Knee Surg Sports Traumatol Arthrosc 25, 2321–2329. [Google Scholar]
- Grasso S, Linklater J, Li Q, Parker DA (2018) Validation of an MRI protocol for routine quantitative assessment of tunnel position in anterior cruciate ligament reconstruction. Am J Sports Med 46, 1624–1631. [Google Scholar]
- Ahn JH, Kim JG, Wang JH, et al. (2012) Long-term results of anterior cruciate ligament reconstruction using bone-patellar tendon-bone: an analysis of the factors affecting the development of osteoarthritis. Arthroscopy 28, 1114–1123. [Google Scholar]
- de Mees TTCR, Reijman M, Waarsing JH, Meuffels DE (2022) Posteriorly positioned femoral grafts decrease long-term failure in anterior cruciate ligament reconstruction, femoral and tibial graft positions did not affect long-term reported outcome. Knee Surg Sports Traumatol Arthrosc 30, 2003–2013. [Google Scholar]
- Pedneault C, Laverdière C, Hart A, et al. (2019) Evaluating the accuracy of tibial tunnel placement after anatomic single-bundle anterior cruciate ligament reconstruction. Am J Sports Med 47, 3187–3194. [Google Scholar]
- Osti M, Krawinkel A, Ostermann M, et al. (2015) Femoral and tibial graft tunnel parameters after transtibial, anteromedial portal, and outside-in single-bundle anterior cruciate ligament reconstruction. Am J Sports Med 43, 2250–2258. [Google Scholar]
- Keenan OJF, Holland G, Maempel JF, et al. (2020) Correlations between radiological classification systems and confirmed cartilage loss in severe knee osteoarthritis. Bone Joint J 102, 301–309. [Google Scholar]
- Cremer P, Peltier A, Maubisson L, et al. (2020) Positioning of the tibial tunnel after single-bundle ACL primary reconstruction on 3D CT scans: a new method. Arthrosc Sports Med Rehabil 2,e615–e622. [Google Scholar]
- Magnussen RA, Debieux P, Benjamin B, et al. (2012) A CT-based classification of prior ACL femoral tunnel location for planning revision ACL surgery. Knee Surg Sports Traumatol Arthrosc 20, 1298–1306. [Google Scholar]
- Warme BA, Ramme AJ, Willey MC, et al. (2012) Reliability of early postoperative radiographic assessment of tunnel placement after anterior cruciate ligament reconstruction. Arthroscopy 28, 942–951. [Google Scholar]
- Shi W-L, Gao Y-T, Zhang K-Y, et al. (2024) Femoral tunnel malposition, increased lateral tibial slope, and decreased notch width index are risk factors for non-traumatic anterior cruciate ligament reconstruction failure. Arthroscopy 40, 424–434-e3. [Google Scholar]
- Asai S, Kim D, Hoshino Y, et al. (2018) Coronal tibial anteromedial tunnel location has minimal effect on knee biomechanics. Knee Surg Sports Traumatol Arthrosc 26, 2960–2965. [Google Scholar]
- Morgan JA, Dahm D, Levy B, et al. (2012) Femoral tunnel malposition in ACL revision reconstruction. J Knee Surg 25, 361–368. [Google Scholar]
- Seo S-S, Kim C-W, Lee C-R, et al. (2019) Effect of femoral tunnel position on stability and clinical outcomes after single-bundle anterior cruciate ligament reconstruction using the outside-in technique. Arthroscopy 35, 1648–1655. [Google Scholar]
- Inoue J, Giusto JD, Dadoo S, et al. (2024) Nonanatomic femoral tunnel placement increases the risk of subsequent meniscal surgery after ACLR: part II-patients without recurrent ACL injury. Knee Surg Sports Traumatol Arthrosc 32, 2780–2789. [Google Scholar]
- Curado J, Hulet C, Hardy P, et al. (2020) Very long-term osteoarthritis rate after anterior cruciate ligament reconstruction: 182 cases with 22-year’ follow-up. Orthop Traumatol Surg Res 106, 459–463. [Google Scholar]
Cite this article as: Erard J, Rarchaert M, Andriollo L, Batailler C, Lustig S & Servien E (2026) Tibial tunnel malposition is a risk factor for osteoarthritis following ACL reconstruction at long term follow up: a retrospective study. SICOT-J 12, 30. https://doi.org/10.1051/sicotj/2026003.
All Tables
a. Distribution of femoral tunnel position. b. Distribution of tibial tunnel position
All Figures
|
Figure 1 3-D CT scan reconstruction of a right tibial plateau axial view. Bony landmarks for ACL footprint and its center (yellow circle and yellow dot) are represented (a, anterior ridge; b, intertubercular fossae; c, medial intercondylar ridge; d, medial border of the lateral groove). |
| In the text | |
|
Figure 2 3-D rCT scan reconstructed images allow assessment of the intra-articular femoral tunnel aperture. a. Distal view. b. Medial view. c. Posterior view. d. Posteromedial view. |
| In the text | |
|
Figure 3 3-D CT scan reconstruction of the right distal femur illustrating the femoral tunnel classification system for the anterior cruciate ligament (ACL). a. Distal view. b. Medial view. c. Posterior view. d. Posteromedial view. Type I tunnels (appropriately positioned or anatomical) are entirely contained within the green zone, located posterior and inferior to the lateral intercondylar ridge (black line). Type II tunnels (slightly malpositioned) partially overlap the lateral intercondylar ridge and extend into the orange zone. Type III tunnels (severely malpositioned or non-anatomical) are positioned completely anterior and superior to the lateral intercondylar ridge, extending into the red zone. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.