| Issue |
SICOT-J
Volume 12, 2026
|
|
|---|---|---|
| Article Number | 20 | |
| Number of page(s) | 7 | |
| Section | Knee | |
| DOI | https://doi.org/10.1051/sicotj/2026020 | |
| Published online | 29 April 2026 | |
Original Article
Implant survival and factors associated with failure of cemented custom-made distal femoral megaprostheses after tumor resection
1
First Department of Orthopaedic Surgery, St. Anne’s University Hospital and Faculty of Medicine, Masaryk University, Brno, Czechia
2
Institute of Solid Mechanics, Mechatronics and Biomechanics, Faculty of Mechanical Engineering, Brno University of Technology, Brno, Czechia
* Corresponding author: This email address is being protected from spambots. You need JavaScript enabled to view it.
Received:
5
March
2026
Accepted:
29
March
2026
Abstract
Background: Distal femoral megaprosthetic reconstruction is a standard limb-salvage procedure after tumor resection. This study aimed to evaluate implant survival and associated factors, the incidence of mechanical failure, and functional outcomes following reconstruction with cemented custom-made distal femoral megaprostheses. Methods: Fifty-seven patients who underwent distal femoral tumor resection followed by reconstruction with a cemented custom-made distal femoral megaprosthesis between 2010 and 2024 were retrospectively analyzed. Implant survival was evaluated using Kaplan–Meier analysis, and associations with outcomes were assessed using Cox proportional hazards and Fine–Gray competing-risk regression models. The analyzed risk factors included age, sex, resection length, stem diameter, fixation length, and functional score. Functional outcomes were assessed using the Musculoskeletal Tumor Society (MSTS) score. Results: Implant survival remained above 60% at the latest follow-up, with survival rates of 100% at 12 months, 93.5% at 24 months, and 72.9% at 60 months. No clinical or implant-related geometric variables were significantly associated with implant survival. The cumulative incidence of mechanical failure was 7% at 48 months and approximately 15% at the latest follow-up, with no association between mechanical failure and resection length, stem diameter, or fixation length. Functional outcomes were favorable, with a mean MSTS score of 21.6 ± 3.9. Conclusion: Cemented custom-made distal femoral megaprostheses demonstrated satisfactory mid- to long-term survival following tumor resection. In this cohort, none of the evaluated variables were significantly associated with implant survival. The incidence of mechanical failure remained relatively low, and geometric implant parameters were not significantly associated with mechanical failure. Functional outcomes were favorable, with most patients achieving good or excellent MSTS scores.
Key words: Distal femur replacement / Megaprosthesis / Bone tumor / Implant survival / Mechanical failure
© The Authors, published by EDP Sciences, 2026
 This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License (https://creativecommons.org/licenses/by/4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Introduction
Distal femoral tumor resection followed by endoprosthetic reconstruction is a mainstay of limb-salvage surgery for primary and metastatic bone tumors of the knee, providing immediate structural stability and facilitating early mobilization [1–3]. Despite advancements in implant design, overall complication rates remain substantial, and implant failure continues to be a significant clinical challenge. Implant failures are commonly categorized by mechanism, with mechanical modes – such as aseptic loosening and structural breakage – representing a relevant subset that may reflect implant design and biomechanical factors [4–6].
Modern practice increasingly favors uncemented fixation techniques because of their potential for biological integration [7]. Cemented custom-made tumor knee endoprostheses are still widely used, particularly in patients with poor bone quality or extensive resection defects, as they provide immediate fixation and mechanical stability [7–9]. However, evidence regarding long-term survival, functional outcomes, and specific mechanical failure patterns in cemented systems remains limited [10–14]. Many existing reports in the literature combine heterogeneous implant types and fixation methods, which obscures the influence of distinct mechanical variables on outcomes [7, 10, 15–17].
Although distal femoral replacement is a well-established reconstructive option after tumor resection, risk factors for implant survival and the influence of geometric implant parameters on outcomes remain insufficiently defined. In particular, the roles of resection length, stem diameter, and fixation length are difficult to assess from the existing literature. By evaluating these parameters in a homogeneous cohort of patients treated with cemented custom-made distal femoral replacements, the present study provides more focused data on implant survival, mechanical failure, and functional outcome in this specific reconstructive setting. The primary aim of this study was to evaluate implant survival and factors associated with implant survival following distal femoral tumor resection reconstructed with cemented custom-made distal femoral megaprostheses. The secondary aim was to assess the incidence and predictors of mechanical failure. A further aim was to describe functional outcomes in this cohort.
Methods
Study design and patients
This retrospective cohort study included 57 patients who underwent distal femoral tumor resection followed by reconstruction with a cemented custom-made distal femoral megaprosthesis (Beznoska) between 2010 and 2024 at a single tertiary referral center. Indications for surgery included primary and metastatic bone tumors of the distal femur. Demographic and tumor characteristics are summarized in Table 1.
Demographic data of patients who underwent tumor resection followed by reconstruction with a cemented custom-made distal femoral megaprosthesis, Beznoska, between 2010 and 2024. Continuous variables are presented as mean ± SD. Categorical variables are presented as number with percentages.
Variables and outcome measures
The primary outcome was implant survival, defined as the time from primary implantation to prosthesis failure for any cause. Implant failure was defined as revision or removal of any prosthetic component. Mechanical failure was defined according to the Henderson classification as type 2 (aseptic loosening) or type 3 (structural failure) [4, 5]. Mechanical variables of interest included length of defect, stem diameter, and fixation length. Length of defect was defined as the distance from the distal femoral joint line to the proximal osteotomy level. Stem diameter was defined as the outer diameter of the femoral intramedullary stem of the megaprosthesis as documented in the implant specification. Length of fixation was defined as the intramedullary length of the femoral stem within the remaining host bone. Measurements of fixation length and defect length were obtained from operative records and postoperative imaging. The femoral stem was implanted using polymethylmethacrylate bone cement with standard cementing technique, including vacuum mixing, pulsatile lavage, retrograde cement insertion, and pressurization. Functional outcome was assessed using the Musculoskeletal Tumor Society (MSTS) [18] score when available. Follow-up assessments were conducted monthly during the first 3 months, every 3 months for the subsequent 2 years, every 6 months until year five, and annually thereafter.
Statistical analysis
Statistical analysis was performed using R (RStudio). Continuous variables are presented as mean ± standard deviation or median (interquartile range), and categorical variables as counts and percentages. Normality was assessed using the Shapiro–Wilk test and graphical methods. A p-value < 0.05 was considered statistically significant. Reverse Kaplan–Meier was used to calculate the median follow-up time. Implant survival was analyzed using the Kaplan–Meier analysis. Associations with outcomes were assessed using Cox proportional hazards regression, with proportionality tested by Schoenfeld residuals. Mechanical failure was additionally analyzed using cumulative incidence functions and competing-risk regression with the Fine–Gray model.
Results
Implant survival and associated factors
Overall implant survival remained above 60% at the latest follow-up, with no clinical or mechanical variables significantly associated with implant survival. Implant survival was 100% at 12 months, 93.5% at 24 months, and 72.9% at 60 months (5 years). A further decline was observed beyond 5 years, with survival remaining above 60% at the latest follow-up. Most failures occurred between 24 and 60 months postoperatively (Figure 1). Failure type distribution is shown in Figure 2.
Univariable Cox regression analysis did not identify any statistically significant predictors of overall implant survival (Table 2). Neither age, length of defect, stem diameter, fixation length, MSTS score, nor sex was associated with an increased risk of implant failure (all p > 0.05).
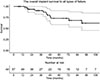 |
Figure 1 Kaplan–Meier curve showing overall implant survival following distal femoral tumor resection, reconstructed with a cemented custom-made distal femoral megaprosthesis. |
 |
Figure 2 Distribution of implant failure types according to the Henderson classification in patients treated with cemented custom-made distal femoral megaprostheses. |
Cox proportional hazards analysis of factors associated with overall implant survival.
Mechanical failure incidence and associated factors
Mechanical failure occurred at a relatively low incidence and was not significantly associated with the evaluated geometric implant parameters. The cumulative incidence of mechanical failure (Henderson types 2 and 3) remained low during the early postoperative period, with no mechanical failures observed within the first 36 months. The cumulative incidence of mechanical failure was 7% at 48 months and increased to 11% at 60 months, reaching approximately 15% at the latest follow-up (Figure 3).
In competing-risk regression analysis using the Fine–Gray model, no mechanical variable was statistically significantly associated with the risk of mechanical failure (Table 3). Length of defect, stem diameter, and fixation length showed no statistically significant association with mechanical failure (all p > 0.05). Representative radiographs of mechanical failure due to aseptic loosening of a cemented custom-made distal femoral megaprosthesis are shown in Figure 4.
 |
Figure 3 Cumulative incidence of mechanical failure (Henderson types 2 and 3) following distal femoral tumor resection reconstructed with a cemented custom-made distal femoral megaprosthesis. |
Competing-risk regression analysis (Fine–Gray model) of factors associated with mechanical failures.
 |
Figure 4 Representative radiographs of cemented custom-made distal femoral megaprosthetic reconstruction after tumor resection. (A) Patient following resection of a conventional grade 2 chondrosarcoma with a 20 cm distal femoral defect reconstructed using a cemented custom-made distal femoral replacement (stem diameter 14 mm, fixation length 21 cm). (B) Patient with malignant epithelioid hemangioendothelioma treated with distal femoral resection of 14 cm and reconstruction using a cemented custom-made megaprosthesis (stem diameter 16 mm, fixation length 17 cm), demonstrating aseptic loosening 6 years after implantation. |
Functional outcomes
Functional outcomes were generally favorable, with most patients achieving good or excellent MSTS scores. Functional outcome assessed using the MSTS score (available in 40 patients) showed a mean score of 21.6 ± 3.9. According to categorical MSTS grading, 45.0% of patients achieved excellent results (76–100%), 47.5% had good outcomes (51–75%), and 7.5% had fair outcomes (26–50%), with no patients classified as having poor (0–25%) functional results.
Discussion
Distal femoral megaprosthetic reconstruction is a widely used limb-salvage procedure following tumor resection, but implant survival and the influence of geometric implant parameters remain incompletely understood. In this study of patients treated with cemented custom-made distal femoral megaprostheses, implant survival remained above 60% at the latest follow-up, mechanical failure occurred at a relatively low incidence, and none of the evaluated geometric parameters – resection length, stem diameter, or fixation length – were significantly associated with implant survival or mechanical failure. Functional outcomes were generally favorable, with most patients achieving good or excellent MSTS scores.
Several limitations should be acknowledged. First, the retrospective design inherently carries the risk of selection and information bias. Second, although the cohort represents a relatively homogeneous group of patients, the sample size remains limited, which may reduce the statistical power to detect subtle associations between mechanical parameters and implant survival. Finally, this study included only cemented custom-made distal femoral megaprostheses from a single institution and manufacturer, which may limit the generalizability of the findings to other implant systems or fixation techniques.
Implant survival in the present cohort was comparable to previously reported outcomes for distal femoral tumor endoprostheses [3, 15, 19–25]. Bergin et al. reported long-term implant survival rates of 73.3% at 10 years and 62.8% at 15 years in patients treated with distal femoral endoprosthetic reconstruction [11]. In a systematic review by Haijie et al., the mean 5-year implant survival rate was 78.3%, compared with 72.9% in our series [19]. Moreover, implant survival remained above 60% at the latest follow-up, supporting the durability of cemented fixation even beyond 5 years in this complex oncologic population. Several studies have identified multiple factors associated with implant survival following distal femoral reconstruction, including patient-related variables, tumor characteristics, and implant design features [3, 15, 19–21, 26]. However, in the present study, none of the evaluated variables – including age, sex, resection length, stem diameter, fixation length, or functional score – were significantly associated with implant survival.
In the present study, the cumulative incidence of mechanical failure remained relatively low, reaching 7% at 48 months and approximately 15% at the latest follow-up. None of the analyzed geometric implant parameters – resection length, stem diameter, or fixation length – were significantly associated with mechanical failure. Reported rates of mechanical failure after distal femoral megaprosthetic reconstruction vary across cohorts but are generally within a comparable range, with mid-term incidences of approximately 5–6% in some series and 5-year implant failure rates around 12–17% in others [10, 11, 27]. Although prior studies report no significant difference between cemented and cementless fixation [19], the delayed onset of mechanical failure in our cohort suggests that cemented fixation provides reliable primary stability, which may be advantageous in patients requiring immediate weight bearing or receiving adjuvant therapy. The lack of an association between resection length and implant survival is noteworthy, as greater resection length has been identified as a major risk factor for aseptic loosening in prior studies [28, 29]. This correlation is typically attributed to increased bending moments and higher stresses at the stem–cement interface in larger resections [11]. Similarly, stem diameter and fixation length, which are commonly considered critical determinants of load distribution and resistance to loosening [19, 28, 29], did not emerge as significant predictors in the present study. The results indicate that mechanical failure in cemented distal femoral megaprostheses is influenced by multiple interacting factors and cannot be determined by simple geometric parameters alone.
Functional outcomes were encouraging, with over 90% of patients achieving good or excellent results according to categorical MSTS grading. The mean MSTS at the most recent follow-up was 21.6 points, which is comparable to previous studies [21, 30]. These findings highlight the ability of distal femoral megaprostheses to restore acceptable limb function and quality of life following extensive tumor resection. Satisfactory functional outcomes were maintained despite substantial defect length, suggesting that the mechanical reconstruction was sufficient to support daily activities. The main findings of selected cohort studies on distal femoral replacement after tumor resection are summarized in Table 4.
Summary of key published cohort studies on cemented distal femoral megaprosthetic reconstruction after tumor resection.
Conclusion
Cemented custom-made distal femoral megaprostheses demonstrated satisfactory mid- to long-term implant survival following tumor resection. In this cohort, none of the evaluated variables were significantly associated with implant survival. The incidence of mechanical failure remained relatively low, and geometric implant parameters were not significantly associated with mechanical failure. Functional outcomes were favorable, with most patients achieving good or excellent MSTS scores. These findings suggest that failure after cemented distal femoral reconstruction is multifactorial and not solely determined by basic geometric implant characteristics.
Funding
This work was supported by the Ministry of Health of The Czech Republic in cooperation with the Czech Health Research Council under project No. NW25-10-00260
Author contribution statement
V. Apostolopoulos: Conceptualization, Methodology, Formal analysis, Writing – original draft. M. Mahdal: Conceptualization, Investigation, Writing – review & editing. M. Kubíček: Investigation, Data curation, Writing – review & editing. L. Pazourek: Investigation, Data curation, Writing – review & editing. P. Boháč: Formal analysis, Methodology, Writing – review & editing. L. Nachtnebl: Supervision, Writing – review & editing. T. Tomáš: Supervision, Investigation, Writing – review & editing.
Conflicts of interest
The authors declare no conflict of interest. The funder had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish these results.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics approval
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Research Ethics Committee of Masaryk University (Brno, Czechia) (Protocol Code: EK-FNUSA-13/2024, date of approval: 12 July 2024). Written informed consent to participate was obtained from all individual participants included in the study.
Informed consent
Written informed consent for publication of their clinical details and any accompanying images was obtained from all participants.
References
- Filis P, Varvarousis D, Ntritsos G, Dimopoulos D, Filis N, Giannakeas N, Korompilias A, Ploumis A (2022) Prosthetic reconstruction following resection of lower extremity bone neoplasms: A systematic review and meta-analysis. J Bone Oncol 36, 100452. [Google Scholar]
- Tsukamoto S, Mavrogenis AF, Masunaga T, Kido A, Honoki K, Tanaka Y, Fujii H, Tanaka Y, Errani C (2023) Megaprosthetic reconstruction of the distal femur with a short residual proximal femur following bone tumor resection: A systematic review. J Orthop Surg Res 18(1), 68. [Google Scholar]
- Houdek MT, Wagner ER, Wilke BK, Wyles CC, Taunton MJ, Sim FH (2016) Long term outcomes of cemented endoprosthetic reconstruction for periarticular tumors of the distal femur. Knee 23(1), 167–172. [Google Scholar]
- Henderson ER, Groundland JS, Pala E, Dennis JA, Wooten R, Cheong D, Windhager R, Kotz RI, Mercuri M, Funovics PT, Hornicek FJ, Temple HT, Ruggieri P, Letson GD (2011) Failure mode classification for tumor endoprostheses: Retrospective review of five institutions and a literature review. J Bone Joint Surg 93(5), 418–429. [CrossRef] [PubMed] [Google Scholar]
- Henderson ER, O’Connor MI, Ruggieri P, Windhager R, Funovics PT, Gibbons CL, Guo W, Hornicek FJ, Temple HT, Letson GD (2014) Classification of failure of limb salvage after reconstructive surgery for bone tumours: A modified system Including biological and expandable reconstructions. Bone Joint J 96-B(11), 1436–1440. [Google Scholar]
- Roustemis AG, Gavriil P, Goumenos S, Trikoupis I, Karampikas V, Koulouvaris P, Kontogeorgakos V, Savvidou O, Mavrogenis AF, Papagelopoulos PJ (2025) Implant survival and risk factors for failure after proximal femoral megaprosthetic reconstruction. SICOT-J 11, 50. [Google Scholar]
- Christ AB, Hornicek FJ, Fabbri N (2021) Distal femoral replacement – Cemented or cementless? Current concepts and review of the literature. J Clin Orthop Trauma 19, 11–16. [Google Scholar]
- Puga TB, Anderson LF, Olfson ER, O’Connor KP, Box MW, Baylak J, Riehl JT (2025) Cemented and uncemented (press-fit) fixation in distal femur replacement (DFR): A systematic review and meta-analysis. Adv Orthop 2, 184–197. [Google Scholar]
- Mellgren A, Tsagkozis P (2025) Outcome of surgical treatment for metastatic bone disease of the distal femur: Observational single-center study of 47 patients. SICOT-J 11, 60. [Google Scholar]
- Holm CE, Bömers JP, Villadsen A, Petersen MM (2025) Evaluation of Zimmer® segmental distal femur mega-prostheses: Patient survival, surgical outcomes and functional outcome. J Bone Oncol 55, 100722. [Google Scholar]
- Bergin PF, Noveau JB, Jelinek JS, Henshaw RM (2012) Aseptic loosening rates in distal femoral endoprostheses: Does stem size matter? Clin Orthop Relat Res 470(3), 743–750. [Google Scholar]
- Schwartz AJ, Kabo JM, Eilber FC, Eilber FR, Eckardt JJ (2010) Cemented distal femoral endoprostheses for musculoskeletal tumor: improved survival of modular versus custom implants. Clin Orthop Relat Res 468(8), 2198–2210. [Google Scholar]
- Tayara B, Nooh A, Chalopin A, Goulding K, Turcotte RE (2021) Outcomes of cemented distal femoral replacement using “line to line” technique with all-polyethylene tibial implant for tumors. J Arthrop 36(8), 2913–2920. [Google Scholar]
- Piakong P, Kiatisevi P, Yau R, Trovarelli G, Lam Y-L, Joyce D, Ruggieri P, Temple HT, Letson D, Binitie O (2020) What is the 10-year survivorship of cemented distal femoral endoprostheses for tumor reconstructions and what radiographic features are associated with survival? Clin Orthop Relat Res 478(11), 2573–2581. [Google Scholar]
- Mazaleyrat M, Le Nail L-R, Auberger G, Biau D, Rosset P, Waast D, Gouin F, Bonnevialle P, Ehlinger M, Pasquier G, Vaz G, French Society of Orthopedic Surgery, Traumatology (SoFCOT) (2020) Survival and complications in hinged knee reconstruction prostheses after distal femoral or proximal tibial tumor resection: A retrospective study of 161 cases. Orthop Traumatol Surg Res 106(3), 403–407. [Google Scholar]
- Dumaine V (2026) Complications of distal femur megaprostheses. Orthop Traumatol Surg Res 112(1), 104527. [Google Scholar]
- Dhawan R, Spencer Jones R, Cool P (2021) Distal femoral replacement – Does length matter? Mid-term results for distal femoral replacements. Knee 31, 97–109. [Google Scholar]
- Enneking WF, Dunham W, Gebhardt MC, Malawar M, Pritchard DJ (1993) A system for the functional evaluation of reconstructive procedures after surgical treatment of tumors of the musculoskeletal system. Clin Orthop Relat Res 286, 241–246. [Google Scholar]
- Haijie L, Dasen L, Tao J, Yi Y, Xiaodong T, Wei G (2018) Implant survival and complication profiles of endoprostheses for treating tumor around the knee in adults: A systematic review of the literature over the past 30 years. J Arthrop 33(4), 1275–1287.e3. [Google Scholar]
- Pala E, Trovarelli G, Angelini A, Maraldi M, Berizzi A, Ruggieri P (2017) Megaprosthesis of the knee in tumor and revision surgery. Acta Biomed 88(2S), 129–138. [Google Scholar]
- Zhang H (2022) Application and development of megaprostheses in limb salvage for bone tumors around the knee joint. Cancer Control 29, 107327482210992. [Google Scholar]
- Ahlmann ER, Menendez LR, Kermani C, Gotha H (2006) Survivorship and clinical outcome of modular endoprosthetic reconstruction for neoplastic disease of the lower limb. J Bone Joint Surg Brit 88-B(6), 790–795. [Google Scholar]
- Jeys LM, Kulkarni A, Grimer RJ, Carter SR, Tillman RM, Abudu A (2008) Endoprosthetic reconstruction for the treatment of musculoskeletal tumors of the appendicular skeleton and pelvis. J Bone Joint Surg 90(6), 1265–1271. [Google Scholar]
- Sharma S, Turcotte RE, Isler MH, Wong C (2006) Cemented rotating hinge endoprosthesis for limb salvage of distal femur tumors. Clin Orthop Relat Res 450, 28–32. [Google Scholar]
- Mattei JC, Chapat B, Ferembach B, Le Nail L-R, Crenn V, Bizzozero P, Venton G, Kerzoncuf M, Loundnou A, Backstein D, Alshaygy I, Griffin A, Wunder J, Biau D, Gouin F, Rosset P, Rochwerger A (2020) Fixed-hinge cemented modular implants: An effective reconstruction technique following primary distal femoral bone tumor resection. A 136-case multicenter series. Orthop Traumatol Surg Res 106(3) 397–402. [Google Scholar]
- Minami N, Tsukamoto S, Shimizu T, Honoki K, Hasegawa H, Masunaga T, Kido A, Errani C, Mavrogenis AF, Tanaka Y (2024) Coverage of lateral soft tissue defects with sartorius muscle flap after distal femoral replacement for malignant bone tumors. SICOT-J 10, 27. [Google Scholar]
- Fiore M, Sambri A, Morante L, Bortoli M, Parisi SC, Panzavolta F, Alesi D, Neri E, Neri MP, Tedeschi S, Zamparini E, Cevolani L, Donati DM, Viale P, Campanacci DA, Zaffagnini S, De Paolis M (2023) Silver-coated distal femur megaprosthesis in chronic infections with severe bone loss: A multicentre case series. JCM 12(20), 6679. [Google Scholar]
- Ruggieri P, Mavrogenis AF, Pala E, Abdel-Mota’al M, Mercuri M (2012) Long term results of fixed-hinge megaprostheses in limb salvage for malignancy. Knee 19 (5), 543–549. [Google Scholar]
- Bus MPA, Van De Sande MAJ, Fiocco M, Schaap GR, Bramer JAM, Dijkstra SPD (2017) What are the long-term results of MUTARS® modular endoprostheses for reconstruction of tumor resection of the distal femur and proximal tibia? Clin Orthop Relat Res 475(3), 708–718. [Google Scholar]
- Jover-Jorge N, González-Rojo P, Amaya-Valero JV, Baixuali-García F, Calva-Ceinós C de la, Angulo-Sánchez MÁ, Lisón JF, Martínez-Gramage J (2024) Evaluating functional outcomes and quality of life in musculoskeletal tumor patients with distal femoral megaprostheses: A case-control study. World J Surg Oncol 22(1), 341. [Google Scholar]
Cite this article as: Apostolopoulos V, Mahdal M, Kubíček M, Pazourek L, Boháč P, Nachtnebl L & Tomáš T (2026) Implant survival and factors associated with failure of cemented custom-made distal femoral megaprostheses after tumor resection. SICOT-J 12, 20. https://doi.org/10.1051/sicotj/2026020.
All Tables
Demographic data of patients who underwent tumor resection followed by reconstruction with a cemented custom-made distal femoral megaprosthesis, Beznoska, between 2010 and 2024. Continuous variables are presented as mean ± SD. Categorical variables are presented as number with percentages.
Cox proportional hazards analysis of factors associated with overall implant survival.
Competing-risk regression analysis (Fine–Gray model) of factors associated with mechanical failures.
Summary of key published cohort studies on cemented distal femoral megaprosthetic reconstruction after tumor resection.
All Figures
|
Figure 1 Kaplan–Meier curve showing overall implant survival following distal femoral tumor resection, reconstructed with a cemented custom-made distal femoral megaprosthesis. |
| In the text | |
|
Figure 2 Distribution of implant failure types according to the Henderson classification in patients treated with cemented custom-made distal femoral megaprostheses. |
| In the text | |
|
Figure 3 Cumulative incidence of mechanical failure (Henderson types 2 and 3) following distal femoral tumor resection reconstructed with a cemented custom-made distal femoral megaprosthesis. |
| In the text | |
|
Figure 4 Representative radiographs of cemented custom-made distal femoral megaprosthetic reconstruction after tumor resection. (A) Patient following resection of a conventional grade 2 chondrosarcoma with a 20 cm distal femoral defect reconstructed using a cemented custom-made distal femoral replacement (stem diameter 14 mm, fixation length 21 cm). (B) Patient with malignant epithelioid hemangioendothelioma treated with distal femoral resection of 14 cm and reconstruction using a cemented custom-made megaprosthesis (stem diameter 16 mm, fixation length 17 cm), demonstrating aseptic loosening 6 years after implantation. |
| In the text | |
Current usage metrics show cumulative count of Article Views (full-text article views including HTML views, PDF and ePub downloads, according to the available data) and Abstracts Views on Vision4Press platform.
Data correspond to usage on the plateform after 2015. The current usage metrics is available 48-96 hours after online publication and is updated daily on week days.
Initial download of the metrics may take a while.